

Comparative effectiveness of sotrovimab and molnupiravir for preventing severe COVID-19 outcomes in patients on kidney replacement therapy: observational study using the OpenSAFELY-UKRR and SRR databases
- PMID: 37915915
- PMCID: PMC10616487
- DOI: 10.1093/ckj/sfad184
Comparative effectiveness of sotrovimab and molnupiravir for preventing severe COVID-19 outcomes in patients on kidney replacement therapy: observational study using the OpenSAFELY-UKRR and SRR databases
Abstract
Background: Due to limited inclusion of patients on kidney replacement therapy (KRT) in clinical trials, the effectiveness of coronavirus disease 2019 (COVID-19) therapies in this population remains unclear. We sought to address this by comparing the effectiveness of sotrovimab against molnupiravir, two commonly used treatments for non-hospitalised KRT patients with COVID-19 in the UK.
Methods: With the approval of National Health Service England, we used routine clinical data from 24 million patients in England within the OpenSAFELY-TPP platform linked to the UK Renal Registry (UKRR) to identify patients on KRT. A Cox proportional hazards model was used to estimate hazard ratios (HRs) of sotrovimab versus molnupiravir with regards to COVID-19-related hospitalisations or deaths in the subsequent 28 days. We also conducted a complementary analysis using data from the Scottish Renal Registry (SRR).
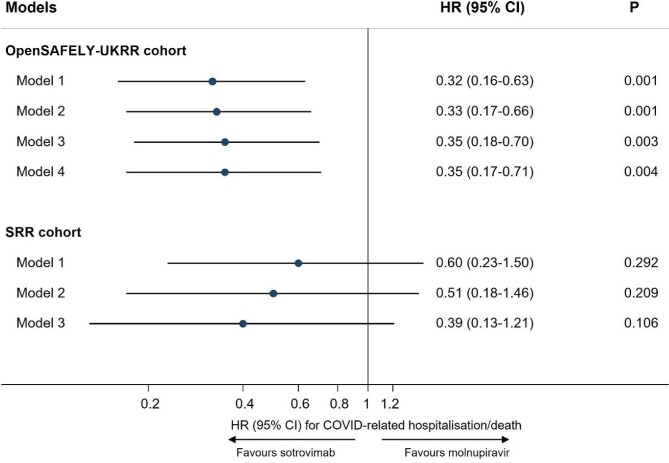
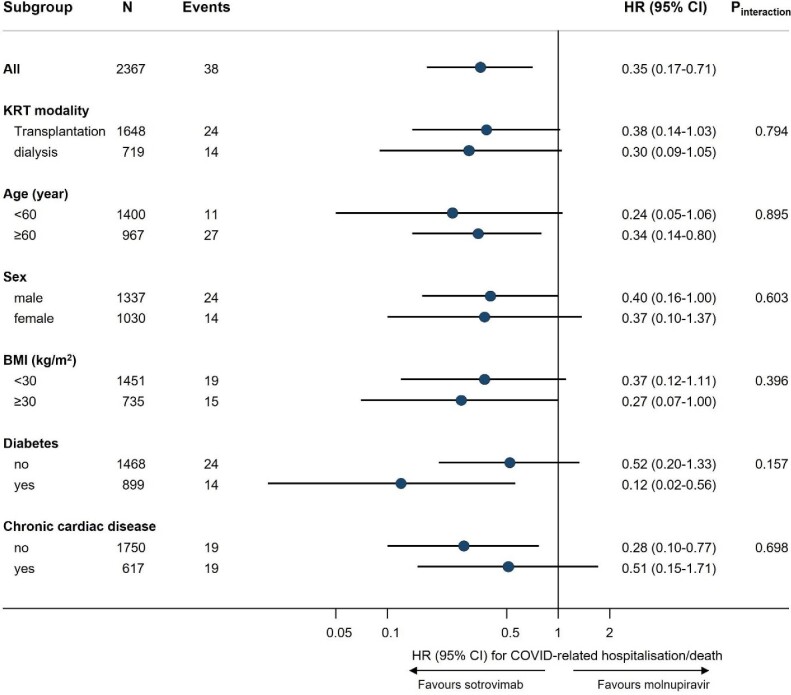
Results: Among the 2367 kidney patients treated with sotrovimab (n = 1852) or molnupiravir (n = 515) between 16 December 2021 and 1 August 2022 in England, 38 cases (1.6%) of COVID-19-related hospitalisations/deaths were observed. Sotrovimab was associated with substantially lower outcome risk than molnupiravir {adjusted HR 0.35 [95% confidence interval (CI) 0.17-0.71]; P = .004}, with results remaining robust in multiple sensitivity analyses. In the SRR cohort, sotrovimab showed a trend toward lower outcome risk than molnupiravir [HR 0.39 (95% CI 0.13-1.21); P = .106]. In both datasets, sotrovimab had no evidence of an association with other hospitalisation/death compared with molnupiravir (HRs ranged from 0.73 to 1.29; P > .05).
Conclusions: In routine care of non-hospitalised patients with COVID-19 on KRT, sotrovimab was associated with a lower risk of severe COVID-19 outcomes compared with molnupiravir during Omicron waves.
Keywords: COVID-19; cohort studies; comparative effectiveness research; renal replacement therapy.
© The Author(s) 2023. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
B.G. has received research funding from the Laura and John Arnold Foundation, NIHR, NIHR School of Primary Care Research, NHS England, NIHR Oxford Biomedical Research Centre, Mohn–Westlake Foundation, NIHR Applied Research Collaboration Oxford and Thames Valley, Wellcome Trust, Good Thinking Foundation, Health Data Research UK, Health Foundation, World Health Organization, UKRI MRC, Asthma UK, British Lung Foundation and the Longitudinal Health and Wellbeing strand of the National Core Studies programme; he is a non-executive director at NHS Digital; he also receives personal income from speaking and writing for lay audiences on the misuse of science. B.M.K. is employed by NHS England, working on medicines policy and a clinical lead for primary care medicines data. A.M. is a member of RCGP health informatics group and the NHS Digital GP data Professional Advisory Group, and received consulting fee from Induction Healthcare. E.P. was a consultant for WHO SAGE COVID-19 Vaccines Working Group. I.J.D. has received research grants from GSK and AstraZeneca and holds shares in GSK. J.T. was funded by an unrestricted grant from GSK for methodological research unrelated to this work. S.L. received remuneration for medical writing from Kidney Care UK, UK Kidney Association and GORE; support for attending meeting from UK Kidney Association; and is Chair of Patients Council of UK Kidney Association, and Secretary and Trustee of Guy's & St Thomas' Kidney Patients' Association. V.M. received grant from National Institute for Health and Care Research. E.C. is a member of UK Kidney Association Infection Prevention & Control committee. F.L. received grants to institution from AstraZeneca, Pfizer, Novartis, and payment to institution from AstraZeneca for scientific events. S.B. received consulting fees from GSK and AstraZeneca. D.N. received grants from National Institute for Health and Care Research, MRC and GSK Open Lab, unrelated to this work; and is the UKKA Director of Informatics Research. L.A.T. has received research funding from MRC, Wellcome, NIHR and GSK, consulted for Bayer in relation to an observational study of chronic kidney disease (unpaid), and is a member of 4 non-industry funded (NIHR/MRC) trial advisory committees (unpaid) and MHRA Expert advisory group (Women's Health). The other authors declare no conflicts of interest.
Figures
References
-
- Nab L, Parker EPK, Andrews CDet al. Changes in COVID-19-related mortality across key demographic and clinical subgroups: an observational cohort study using the OpenSAFELY platform on 18 million adults in England. Lancet Public Health 2023;8:E364–77. 10.1016/S2468-2667(23)00079-8 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
