

Copeptin, Natriuretic Peptides, and Cardiovascular Outcomes in Patients With CKD: The German Chronic Kidney Disease (GCKD) Study
- PMID: 37915964
- PMCID: PMC10616426
- DOI: 10.1016/j.xkme.2023.100725
Copeptin, Natriuretic Peptides, and Cardiovascular Outcomes in Patients With CKD: The German Chronic Kidney Disease (GCKD) Study
Abstract
Rationale & objective: Copeptin and Midrange pro-atrial natriuretic peptide (MR-pro-ANP) are associated with outcomes independently of N-terminal pro-brain natriuretic peptide (NT-pro-BNP) in patients with heart failure (HF). The value of these markers in patients with chronic kidney disease (CKD) has not been studied.
Study design: Prospective cohort study.
Setting & participants: A total of 4,417 patients enrolled in the German Chronic Kidney Disease (GCKD) study with an estimated glomerular filtration rate of 30-60 mL/min/1.73m2 or overt proteinuria (urinary albumin-creatinine ratio >300mg/g or equivalent).
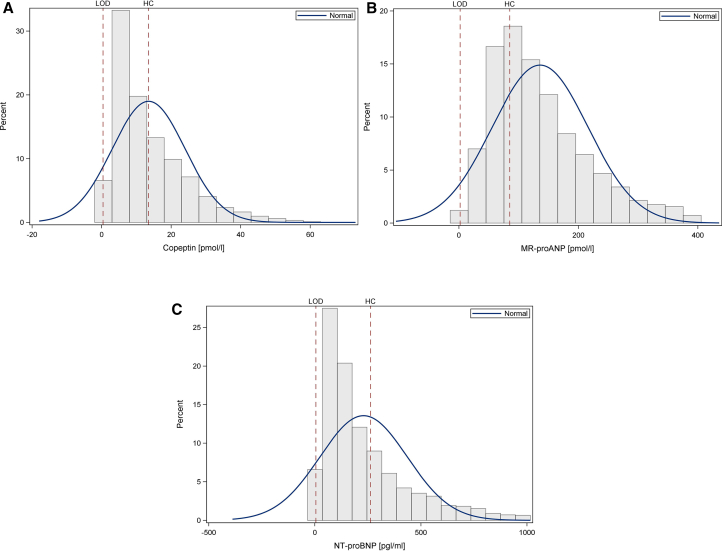
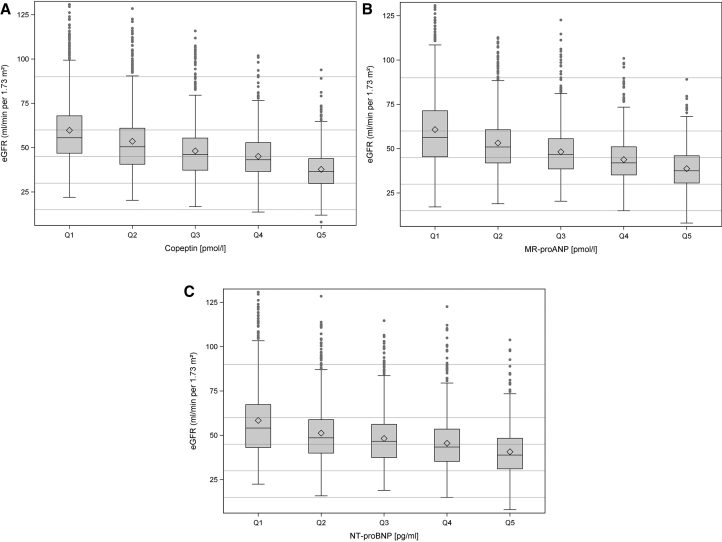
Exposures: Copeptin, MR-pro-ANP, and NT-pro-BNP levels were measured in baseline samples.
Outcomes: Noncardiovascular death, cardiovascular (CV) death, major adverse CV event (MACE), and hospitalization for HF.
Analytical approach: HRs for associations of Copeptin, MR-pro-ANP, and NT-pro-BNP with outcomes were estimated using Cox regression analyses adjusted for established risk factors.
Results: During a maximum follow-up of 6.5 years, 413 non-CV deaths, 179 CV deaths, 519 MACE, and 388 hospitalizations for HF were observed. In Cox regression analyses adjusted for established risk factors, each one of the 3 markers were associated with all the 4 outcomes, albeit the highest HRs were found for NT-pro-BNP. When models were extended to include all the 3 markers, NT-pro-BNP remained associated with all 4 outcomes. Conversely, from the 2 novel markers, associations remained only for Copeptin with non-CV death (HR, 1.62; 95% CI, 1.04-2.54 for highest vs lowest quintile) and with hospitalizations for HF (HR, 1.73; 95% CI, 1.08-2.75).
Limitations: Single-point measurements of Copeptin, MR-pro-ANP, and NT-pro-BNP.
Conclusions: In patients with moderately severe CKD, we confirm NT-pro-BNP to be strongly associated with all outcomes examined. As the main finding, the novel marker Copeptin demonstrated independent associations with non-CV death and hospitalizations for HF, and should therefore be evaluated further for risk assessment in CKD.
Plain-language summary: A blood sample-based biomarker that indicates high cardiovascular risk in a patient with kidney disease would help to guide interventions and has the potential to improve outcomes. In 4,417 patients of the German Chronic Kidney Disease study, we assessed the relationship of Copeptin, pro-atrial natriuretic peptide, and N-terminal pro-brain natriuretic peptide (NT-pro-BNP) with important outcomes over a follow-up period of 6.5 years. NT-pro-BNP was strongly associated with all of the 4 outcomes, including death unrelated to cardiovascular disease, death because of cardiovascular disease, a major cardiovascular event, and hospitalization for heart failure. Copeptin was associated with death unrelated to cardiovascular disease and hospitalization for heart failure. NT-pro-BNP and Copeptin are, therefore, promising candidates for a blood sample-based strategy to identify patients with kidney disease at high cardiovascular risk.
Keywords: Copeptin; MR-pro-ANP; NT-pro-BNP; biomarkers; cardiac diseases; chronic kidney disease; heart failure; kidney diseases.
© 2023 The Authors.
Figures
References
-
- Foreman K.J., Marquez N., Dolgert A., et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet. 2018;392(10159):2052–2090. doi: 10.1016/S0140-6736(18)31694-5. - DOI - PMC - PubMed
-
- von Haehling S., Jankowska E.A., Morgenthaler N.G., et al. Comparison of midregional pro-atrial natriuretic peptide with N-terminal pro-B-type natriuretic peptide in predicting survival in patients with chronic heart failure. J Am Coll Cardiol. 2007;50(20):1973–1980. doi: 10.1016/j.jacc.2007.08.012. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
