Cost-Effectiveness Analysis of Myopia Progression Interventions in Children
- PMID: 37917061
- PMCID: PMC10623196
- DOI: 10.1001/jamanetworkopen.2023.40986
Cost-Effectiveness Analysis of Myopia Progression Interventions in Children
Erratum in
-
Error in Discussion.JAMA Netw Open. 2025 May 1;8(5):e2518553. doi: 10.1001/jamanetworkopen.2025.18553. JAMA Netw Open. 2025. PMID: 40434781 Free PMC article. No abstract available.
Abstract
Importance: Several interventions exist for treating myopia progression in children. While these interventions' efficacy has been studied, their cost-effectiveness remains unknown and has not been compared.
Objective: To determine cost-effective options for controlling myopia progression in children.
Design, setting, and participants: In this cost-effectiveness analysis, a Markov model was designed to compare the cost-effectiveness of interventions for controlling myopia progression over 5 years from a societal perspective in a simulated hypothetical cohort of patients aged 10 years with myopia. Myopia interventions considered included atropine eye drops, 0.05% and 0.01%, defocus incorporated multiple segment spectacles, outdoor activity, soft contact lenses (daily disposable and multifocal), rigid gas-permeable contact lenses, progressive addition lenses, bifocal spectacle lenses, orthokeratology, highly aspherical lenslets (HALs), and red light therapy; all interventions were compared with single-vision lenses. Deterministic and probabilistic sensitivity analysis determined the association of model uncertainties with the cost-effectiveness. Costs were obtained from the charges of the Hospital Authority of Hong Kong and The Chinese University of Hong Kong Eye Center.
Main outcome and measures: The mean costs (in US dollars) per child included the cost of hospital visits, medications, and optical lenses. The outcomes of effectiveness were the annual spherical equivalent refraction (SER) and axial length (AL) reductions. Incremental cost-effectiveness ratios (ICERs) were calculated for each strategy relative to single-vision lenses over a time horizon of 5 years.
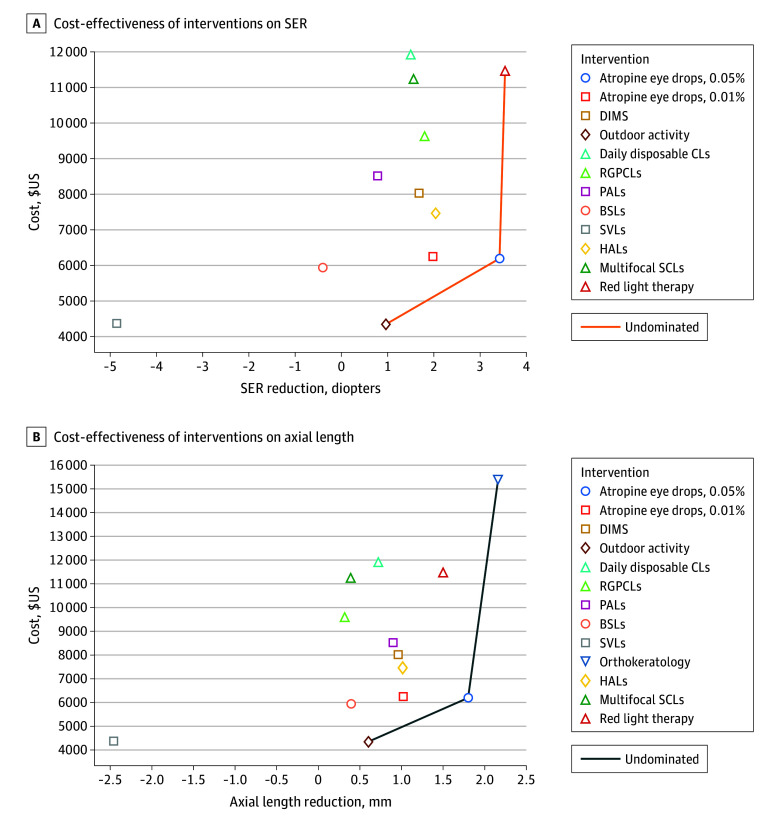
Results: Outdoor activity, atropine (0.05%), red light therapy, HALs, and orthokeratology were cost-effective. The ICER of atropine, 0.05%, was US $220/SER reduction; red light therapy, US $846/SER reduction; and HALs, US $448/SER reduction. Outdoor activity yielded a savings of US $5/SER reduction and US $8/AL reduction. Orthokeratology resulted in an ICER of US $2376/AL reduction.
Conclusions and relevance: These findings suggest that atropine eye drops, 0.05%, and outdoor activity are cost-effective for controlling myopia progression in children. Though more expensive, red light therapy, HALs, and orthokeratology may also be cost-effective. The use of these interventions may help to control myopia in a cost-effective way.
Conflict of interest statement
Figures