

Bernese periacetabular osteotomy (PAO): from its local inception to its worldwide adoption
- PMID: 37917385
- PMCID: PMC10622391
- DOI: 10.1186/s10195-023-00734-2
Bernese periacetabular osteotomy (PAO): from its local inception to its worldwide adoption
Abstract
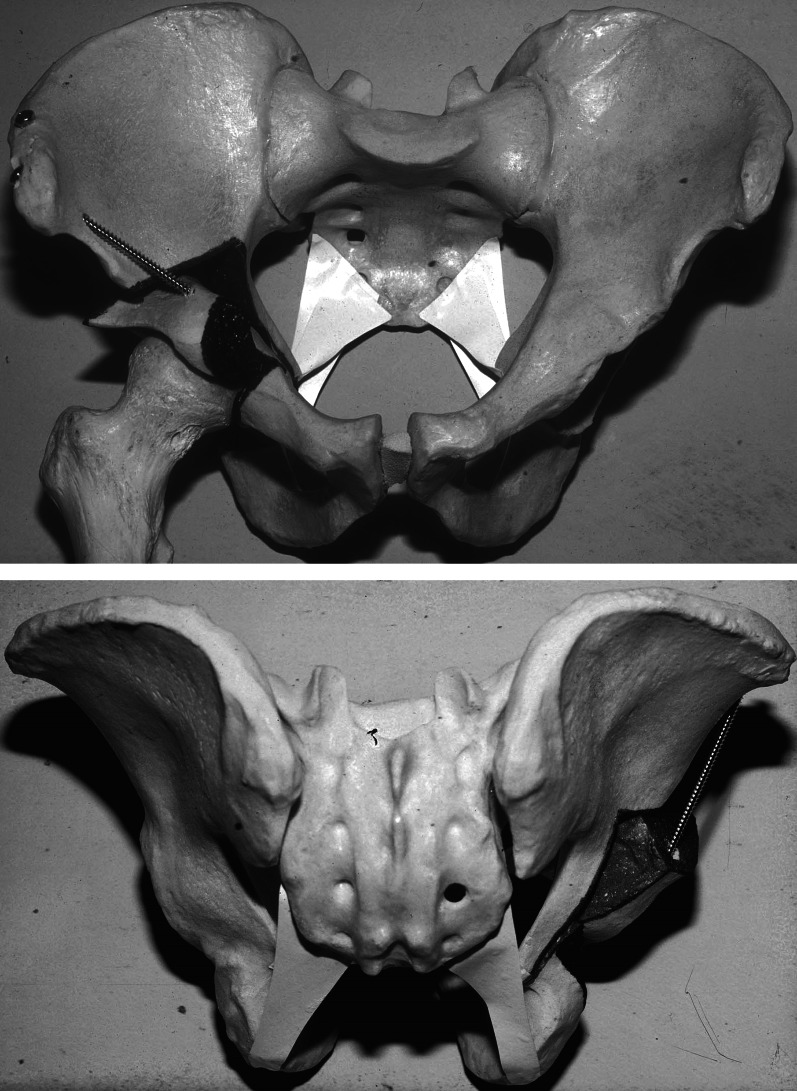
The development of the Bernese periacetabular osteotomy (PAO) is based on a structured approach starting with an analysis of the preexisting procedures to improve the coverage of the femoral head and was followed by a list of additional goals and improvements. Cadaveric dissections with a detailed description of the vascular supply of acetabulum and periacetabular bone set the stage for an intrapelvic approach, which offered the largest acetabular correction possible combined with safe intracapsular access. The final composition of osteotomies required the development of several instruments and cutting devices before the feasibility could be tested on a series of cadaveric hips.While the sequence of the osteotomies remained largely unchanged over time (except for the pubic and ischial osteotomies), several propositions for an easier/less invasive approach have been discussed; some made it into standard practice. Efforts were undertaken to optimize the learning curve and minimize failures using video-clips, hands-on courses, fellowships, publications, and ongoing mentoring programs. In retrospect, with almost 40 years of experience, such efforts have promoted a worldwide adoption of the Bernese periacetabular osteotomy.
Keywords: Bernese PAO; Hip joint preservation surgery; PAO; Pelvic osteotomy history; Periacetabular osteotomy.
© 2023. The Author(s).
Conflict of interest statement
All the authors declare that they have no affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest, in the subject matter or materials discussed in this manuscript.
Figures










References
-
- Codivilla A. Operative treatment of congenital dislocation of the hip. Z Orthop Chir. 1901;9:124–137.
-
- Codivilla A. The operative treatment of congenital dislocations. New York Medical J. 1902;73:741.
-
- Colonna PC. Congenital dislocation of the hips in older subjects: based on a study of sixty-six open operations. J Bone Joint Surg. 1932;14:277–298.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
