

Screening for mitochondrial function before use-routine liver assessment during hypothermic oxygenated perfusion impacts liver utilization
- PMID: 37918219
- PMCID: PMC10641151
- DOI: 10.1016/j.ebiom.2023.104857
Screening for mitochondrial function before use-routine liver assessment during hypothermic oxygenated perfusion impacts liver utilization
Abstract
Background: To report on a concept of liver assessment during ex situ hypothermic oxygenated perfusion (HOPE) and its significant impact on liver utilization.
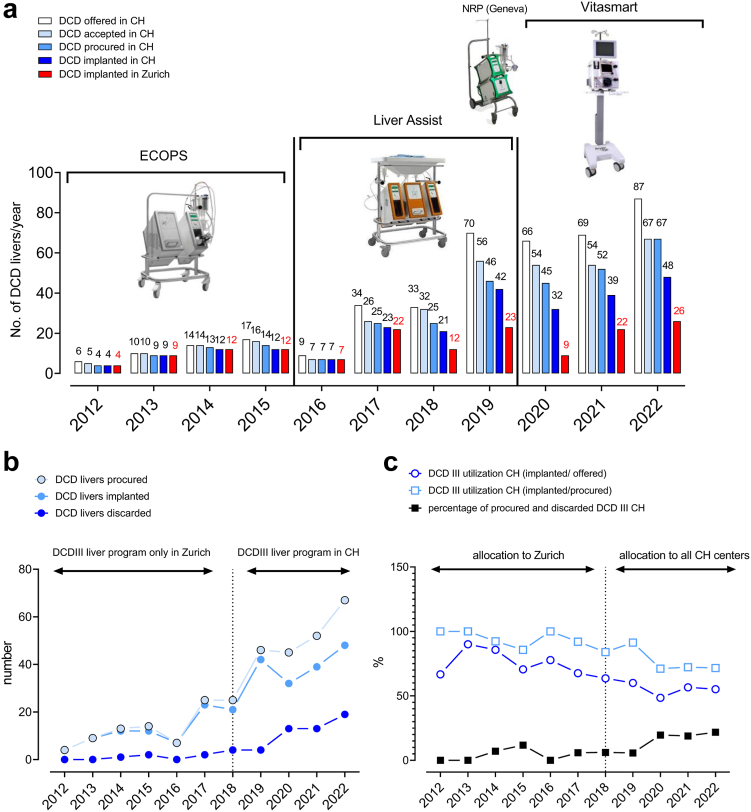
Methods: An analysis of prospectively collected data on donation after circulatory death (DCD) livers, treated by HOPE at our institution, during a 11-year period between January 2012 and December 2022.
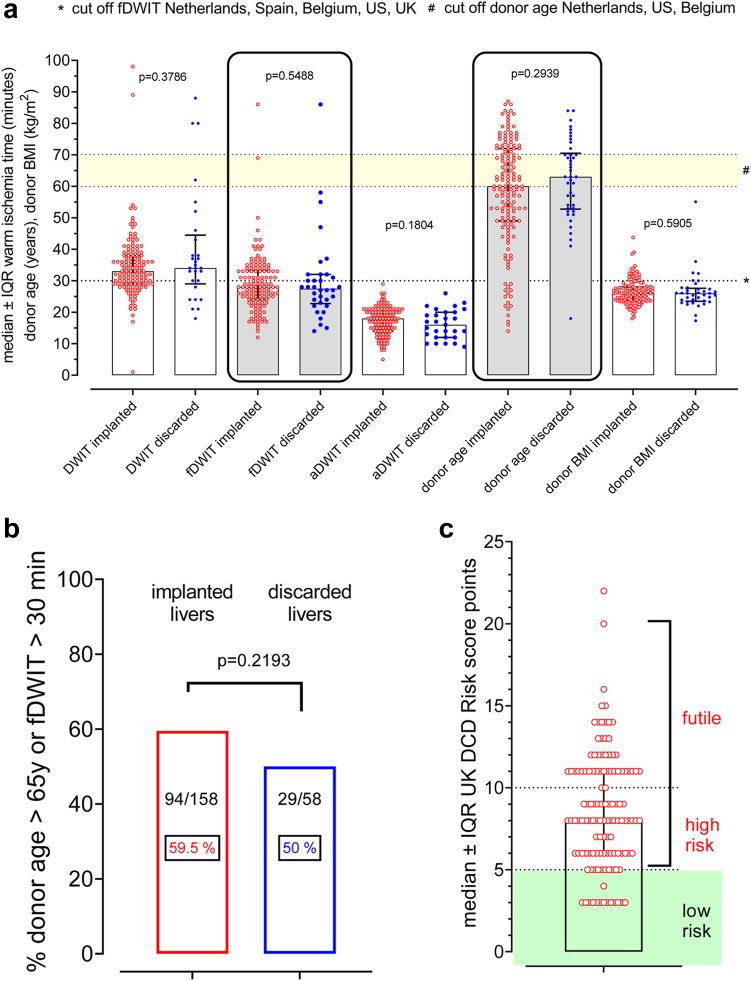
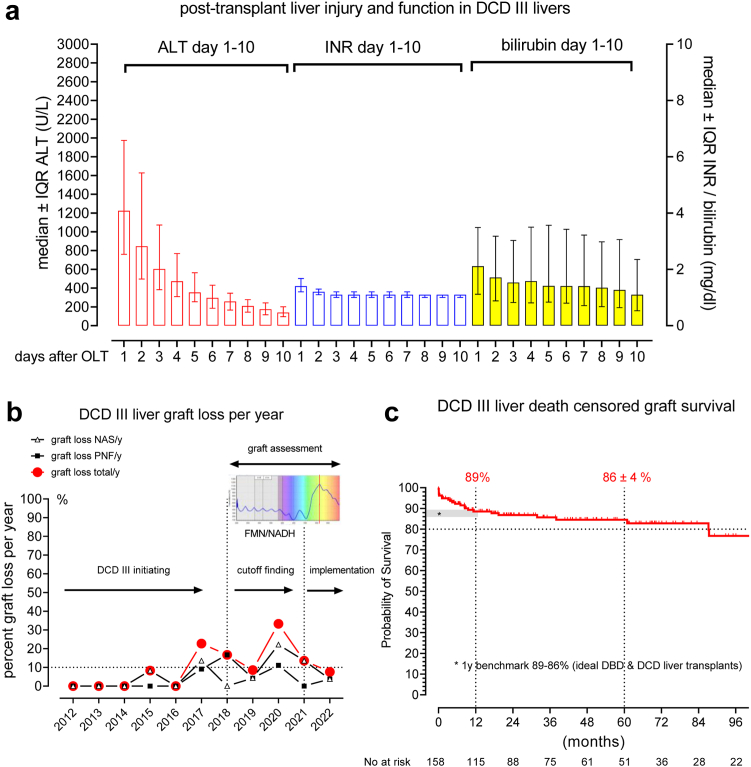
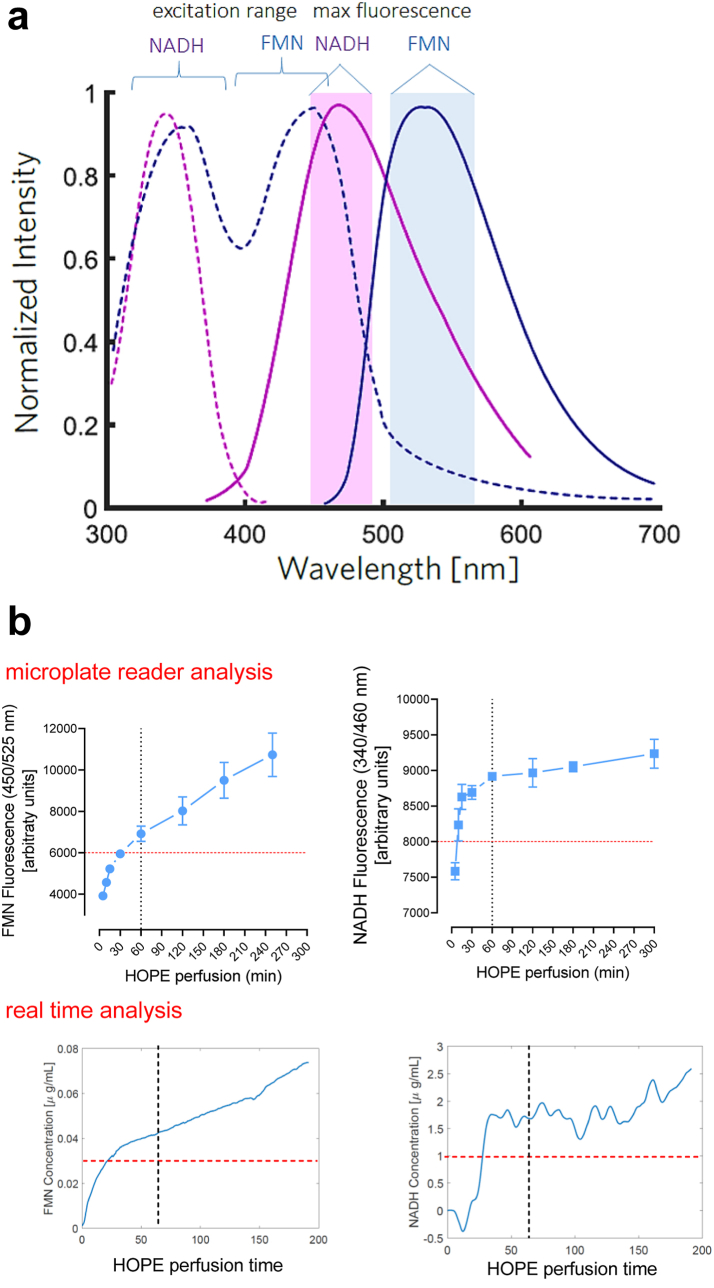
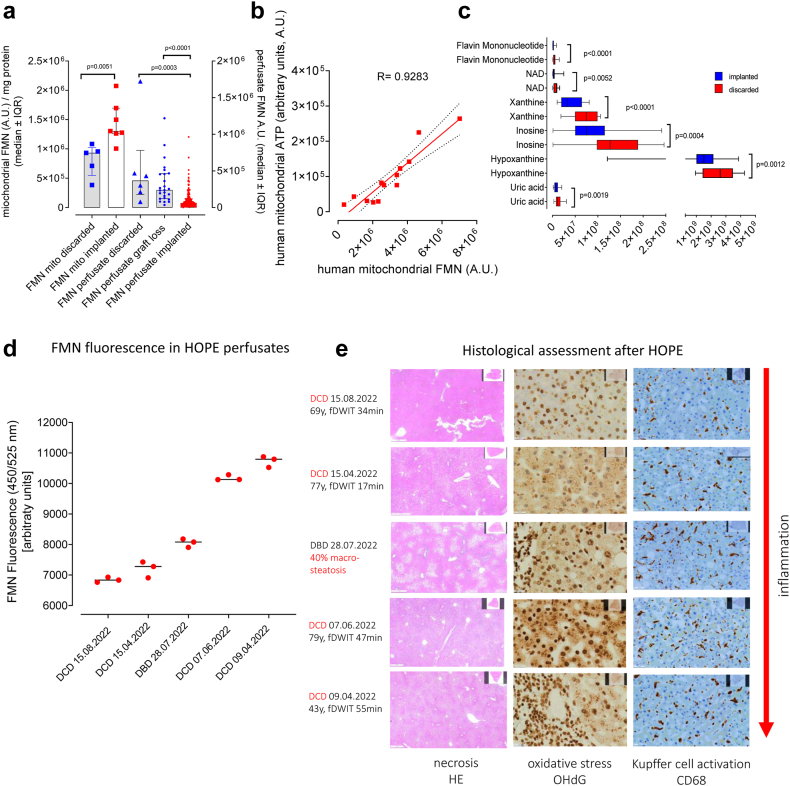
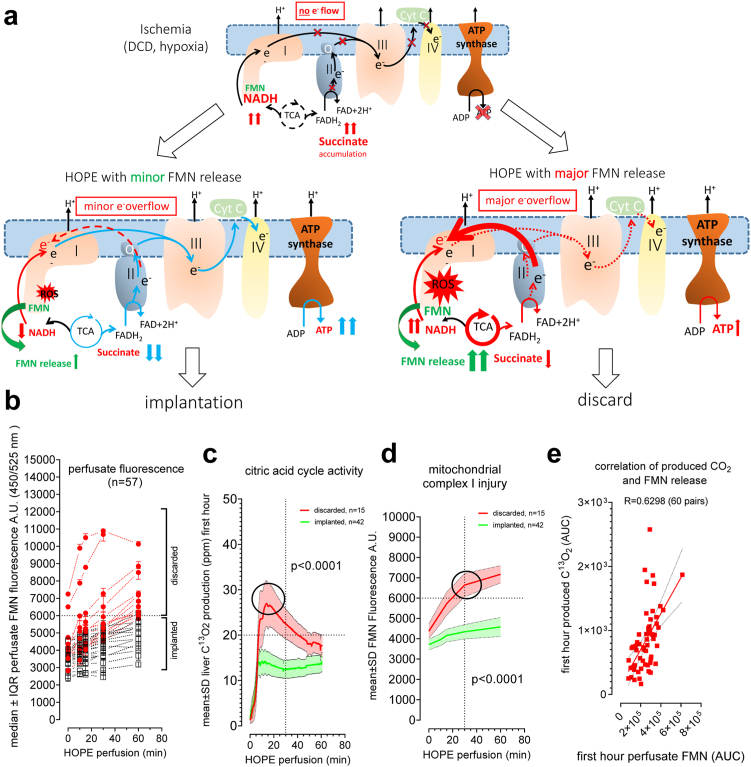
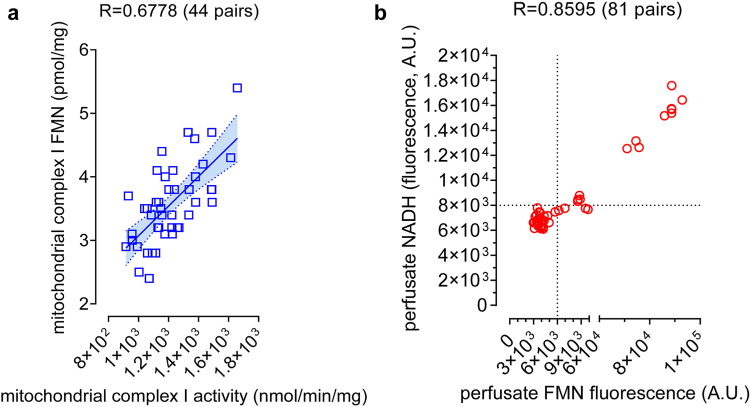
Findings: Four hundred and fifteen DCD Maastricht III livers were offered during the study period in Switzerland, resulting in 249 liver transplants. Of those, we performed 158 DCD III liver transplants at our institution, with 1-year patient survival and death censored graft survival (death with functioning graft) of 87 and 89%, respectively, thus comparable to benchmark graft survivals of ideal DBD and DCD liver transplants (89% and 86%). Correspondingly, graft loss for primary non-function or cholangiopathy was overall low, i.e., 7/158 (4.4%) and 11/158 (6.9%), despite more than 82% of DCD liver grafts ranked high (6-10 points) or futile risk (>10 points) according to the UK-DCD score. Consistently, death censored graft survival was not different between low-, high-risk or futile DCD III livers. The key behind these achievements was the careful development and implementation of a routine perfusate assessment of mitochondrial biomarkers for injury and function, i.e., release of flavin mononucleotide from complex I, perfusate NADH, and mitochondrial CO2 production during HOPE, allowing a more objective interpretation of liver quality on a subcellular level, compared to donor derived data.
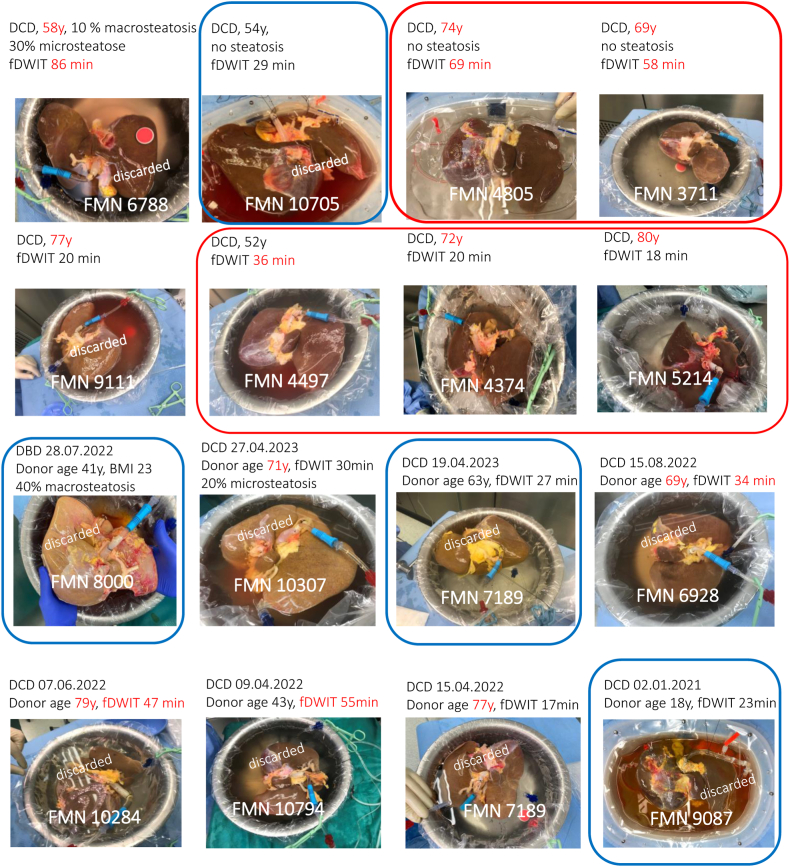
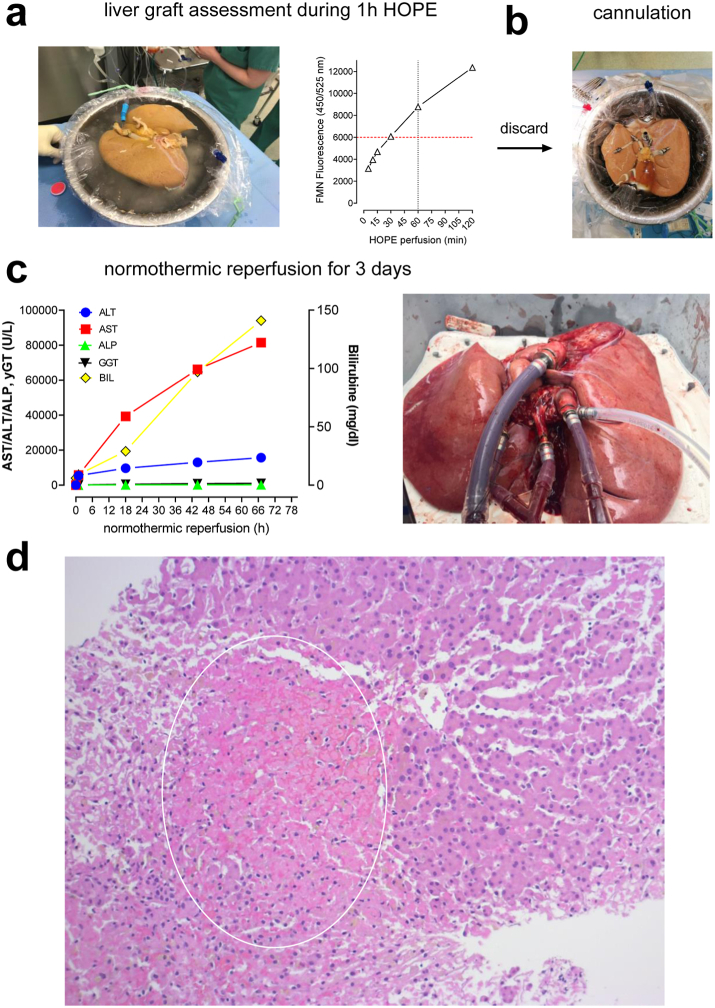
Interpretation: HOPE after cold storage is a highly suitable and easy to perform perfusion approach, which allows reliable liver graft assessment, enabling surgeons to make a fact based decision on whether or not to implant the organ. HOPE-treatment should be combined with viability assessment particularly when used for high-risk organs, including DCD livers or organs with relevant steatosis.
Funding: This study was supported by the Swiss National Foundation (SNF) grant 320030_189055/1 to PD.
Keywords: Donation after circulatory death; Flavin mononucleotide; Hypothermic oxygenated perfusion; Liver utilization.
Copyright © 2023 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests A.S. received consultant fees for presentations from Bridge to life LTD, all other authors declare no competing interests.
Figures
References
-
- Eden J., Sousa Da Silva R., Cortes-Cerisuelo M., et al. Utilization of livers donated after circulatory death for transplantation–an international comparison. J Hepatol. 2023;78:1007–1016. - PubMed
-
- Muller X., Schlegel A., Kron P., et al. Novel real-time prediction of liver graft function during hypothermic oxygenated machine perfusion before liver transplantation. Ann Surg. 2019;270:783–790. - PubMed
-
- de Rougemont O., Breitenstein S., Leskosek B., et al. One hour hypothermic oxygenated perfusion (HOPE) protects nonviable liver allografts donated after cardiac death. Ann Surg. 2009;250:674–683. - PubMed
-
- Schlegel A., van Reeven M., Croome K., et al. A multicentre outcome analysis to define global benchmarks for donation after circulatory death liver transplantation. J Hepatol. 2022;76:371–382. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
