

Direct comparison of digital subtraction myelography versus CT myelography in lateral decubitus position: evaluation of diagnostic yield for cerebrospinal fluid-venous fistulas
- PMID: 37918908
- PMCID: PMC11420736
- DOI: 10.1136/jnis-2023-020789
Direct comparison of digital subtraction myelography versus CT myelography in lateral decubitus position: evaluation of diagnostic yield for cerebrospinal fluid-venous fistulas
Abstract
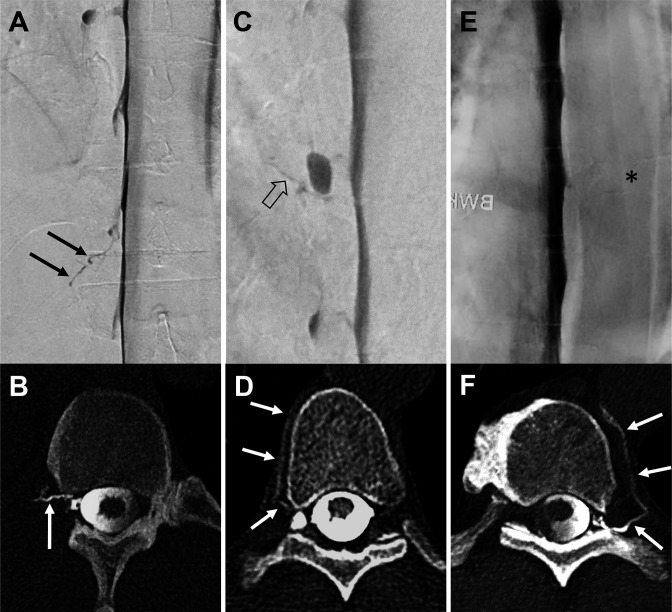
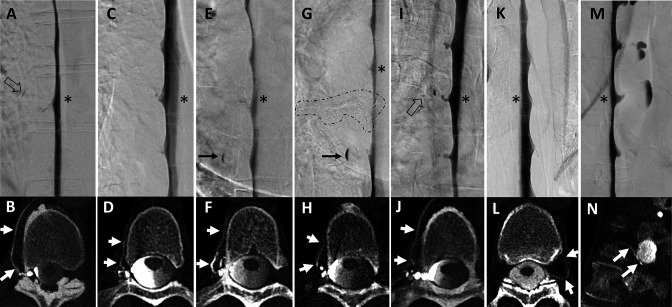
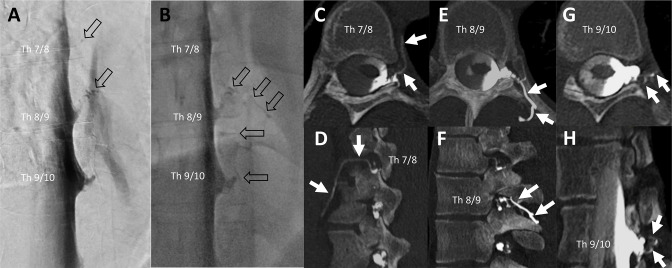
Background: Cerebrospinal fluid (CSF)-venous fistulas (CVFs) are increasingly identified as a cause of spontaneous intracranial hypotension (SIH). Lateral decubitus digital subtraction myelography (LD-DSM) and CT myelography (LD-CTM) are mainly used for detection, but the most sensitive method is yet unknown.
Objective: To compare LD-DSM with LD-CTM for diagnostic yield of CVFs.
Methods: Patients with SIH diagnosed with a CVF between January 2021 and December 2022 in which the area of CVF(s) was covered by both diagnostic modalities were included. LD-CTM immediately followed LD-DSM without repositioning the spinal needle, and the second half of the contrast agent was injected at the CT scanner. Patients were awake or mildly sedated. Retrospectively, two neuroradiologists evaluated data independently and blinded for the presence of CVF.
Results: Twenty patients underwent a total of 27 combined LD-DSM/LD-CTM examinations (4/20 with follow-up and 3/20 with bilateral examinations). Both raters identified significantly more CVFs with LD-CTM than with LD-DSM (rater 1: 39 vs 9, P<0.001; rater 2: 42 vs 12, P<0.001). Inter-rater agreement was substantial for LD-DSM (κ=0.732) and LD-CTM (κ=0.655). The results remained significant after considering the senior rating for cases of disagreement (39 vs 10; P<0.001), and no CVF detected on LD-DSM was missed on LD-CTM.
Conclusion: In this study, LD-CTM has a higher diagnostic yield for the detection of CVFs than LD-DSM and should supplement LD-DSM, but further studies are needed. LD-CTM can be easily acquired in awake or mildly sedated patients with the second half of contrast injected just before CT scanning, or it may be considered as a stand-alone investigation.
Keywords: CT; Intervention; Spine.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials