

Distinct receptor binding domain IgG thresholds predict protective host immunity across SARS-CoV-2 variants and time
- PMID: 37919289
- PMCID: PMC10622572
- DOI: 10.1038/s41467-023-42717-1
Distinct receptor binding domain IgG thresholds predict protective host immunity across SARS-CoV-2 variants and time
Abstract
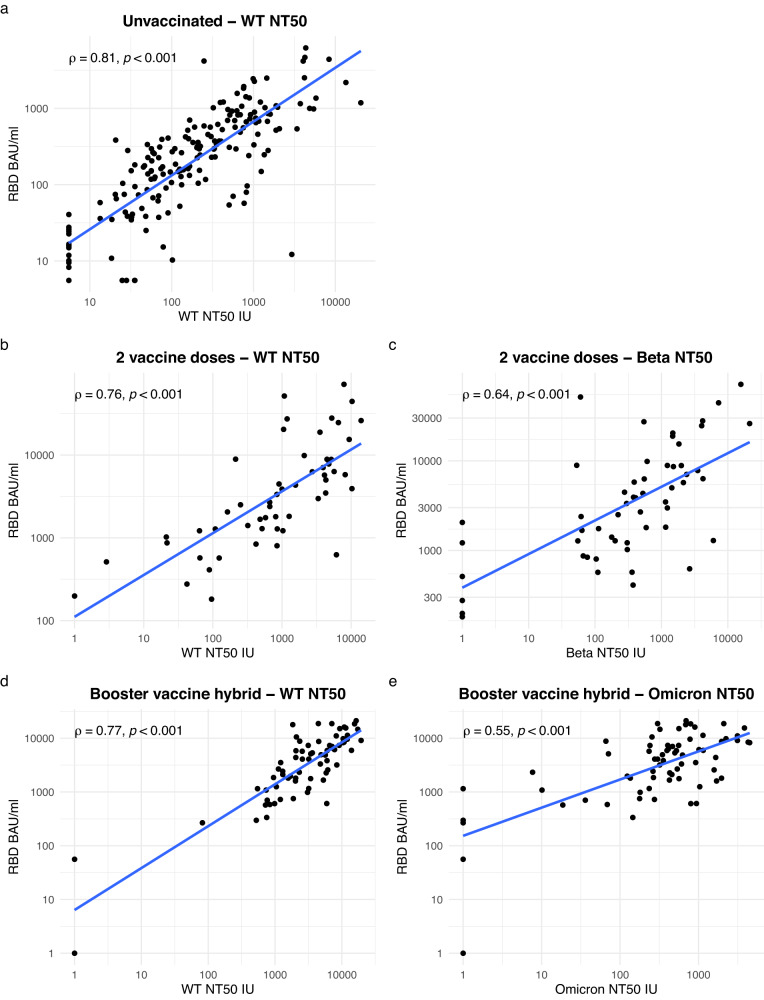
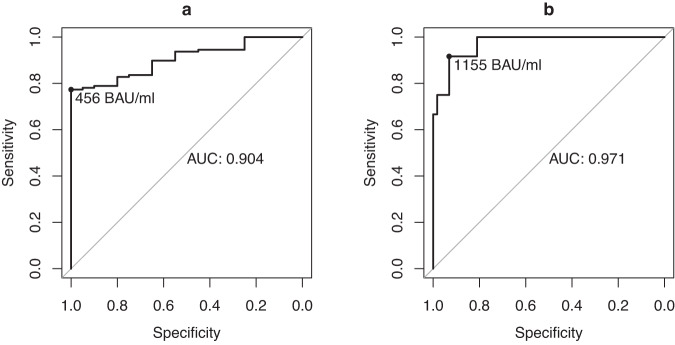
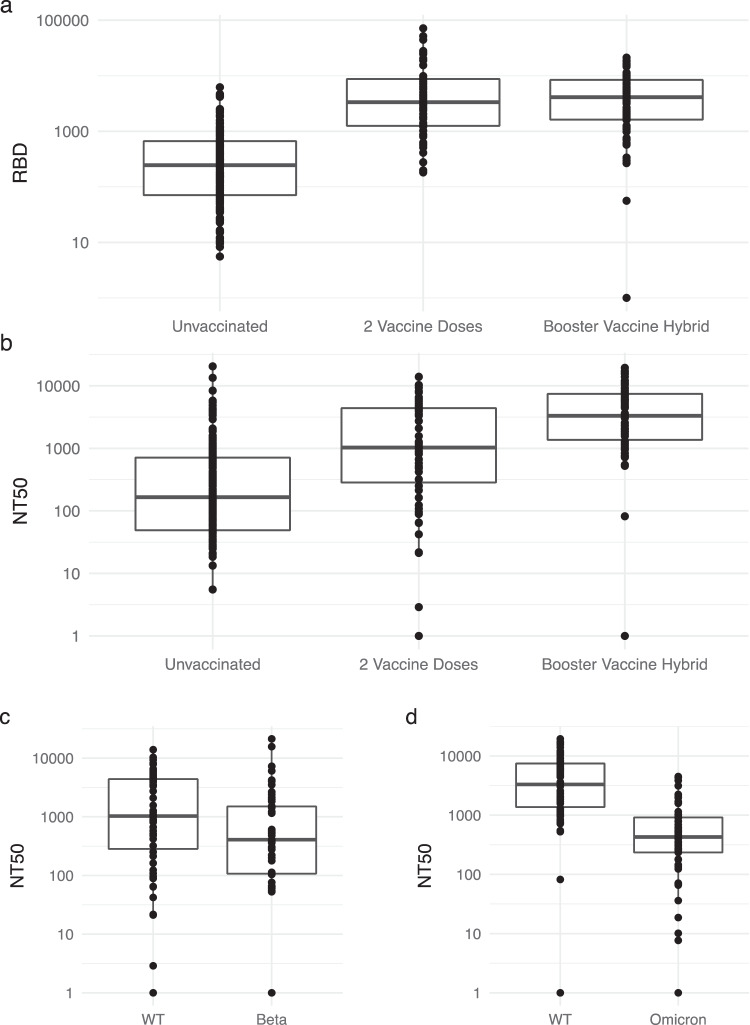
SARS-CoV-2 neutralising antibodies provide protection against COVID-19. Evidence from early vaccine trials suggested binding antibody thresholds could serve as surrogate markers of neutralising capacity, but whether these thresholds predict sufficient neutralising capacity against variants of concern (VOCs), and whether this is impacted by vaccine or infection history remains unclear. Here we analyse individuals recovered from, vaccinated or with hybrid immunity against SARS-CoV-2. An NT50 ≥ 100 IU confers protection in vaccine trials, however, as VOC induce a reduction in NT50, we use NT50 ≥ 1000 IU as a cut off for WT NT50 that would retain neutralisation against VOC. In unvaccinated convalescent participants, a receptor binding domain (RBD) IgG of 456 BAU/mL predicts an NT50 against WT of 1000 IU with an accuracy of 80% (95%CI 73-86%). This threshold maintains accuracy in determining loss of protective immunity against VOC in two vaccinated cohorts. It predicts an NT50 < 100 IU against Beta with an accuracy of 80% (95%CI 67-89%) in 2 vaccine dose recipients. In booster vaccine recipients with a history of COVID-19 (hybrid immunity), accuracy is 87% (95%CI 77-94%) in determining an NT50 of <100 IU against BA.5. This analysis provides a discrete threshold that could be used in future clinical studies.
© 2023. The Author(s).
Conflict of interest statement
E.F. has received consulting fees from Gilead, ViiV and Vidacare Ireland, and has been awarded a grant from Science Foundation Ireland outside the submitted work. E.d.B. has received consulting fees from Sanofi Pasteur and an honoraria/travel grant from Pfizer. P.M. has received honoraria and/or travel grants from Gilead Sciences, MSD, Astrazeneca, and ViiV Healthcare, and has been awarded grants by Science Foundation Ireland outside the submitted work. P.K. reports grants or contracts from German Federal Ministry of Research and Education (BMBF) B-FAST (Bundesweites Forschungsnetz Angewandte Surveillance und Testung) and NAPKON (Nationales Pandemie Kohorten Netz, German National Pandemic Cohort Network) of the Network University Medicine (NUM) and the State of North Rhine-Westphalia; Consulting fees Ambu GmbH, Gilead Sciences, Mundipharma Research Limited, Noxxon N.V. and Pfizer Pharma; Honoraria for lectures from Akademie für Infektionsmedizin e.V., Ambu GmbH, Astellas Pharma, BioRad Laboratories Inc., Datamed GmbH, European Confederation of Medical Mycology, Gilead Sciences, GPR Academy Ruesselsheim, HELIOS Kliniken GmbH, Lahn-Dill-Kliniken GmbH, medupdate GmbH, MedMedia GmbH, MSD Sharp & Dohme GmbH, Pfizer Pharma GmbH, Scilink Comunicación Científica SC, streamedup! GmbH and University Hospital and LMU Munich; Participation on an Advisory Board from Ambu GmbH, Gilead Sciences, Mundipharma Research Limited and Pfizer Pharma; A pending patent currently reviewed at the German Patent and Trade Mark Office (DE 10 2021 113 007.7); Other non-financial interests from Elsevier, Wiley and Taylor & Francis online outside the submitted work. J.S. has received research support from the German Federal Ministry of Education and Research (BMBF) and Basilea Pharmaceuticals Inc.; has received speaker honoraria by Pfizer Inc., Gilead, and AbbVie; has been a consultant to Gilead, Produkt&Markt GmbH, Alvea Vax. and Micron Research and has received travel grants by German Society for Infectious Diseases (DGI e.V.) and Meta-Alexander Foundation. O.A.C. reports grants or contracts from BMBF, Cidara, EU-DG RTD (101037867), Pfizer; Consulting fees from Biocon, Biosys, Janssen, Noxxon, Pfizer; Honoraria for lectures from Gilead, MedScape, Merck/MSD, Pfizer; Participation on a Data Safety Monitoring Board or Advisory Board from Cidara, Janssen. A.L. receives consulting fees from Abbott and is co-chair of the Gilead Research Scholars Programme. All other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
