

Gut microbiota composition and diversity before, during, and two months after rifamycin-based tuberculosis preventive therapy
- PMID: 37919333
- PMCID: PMC10622450
- DOI: 10.1038/s41598-023-44854-5
Gut microbiota composition and diversity before, during, and two months after rifamycin-based tuberculosis preventive therapy
Abstract
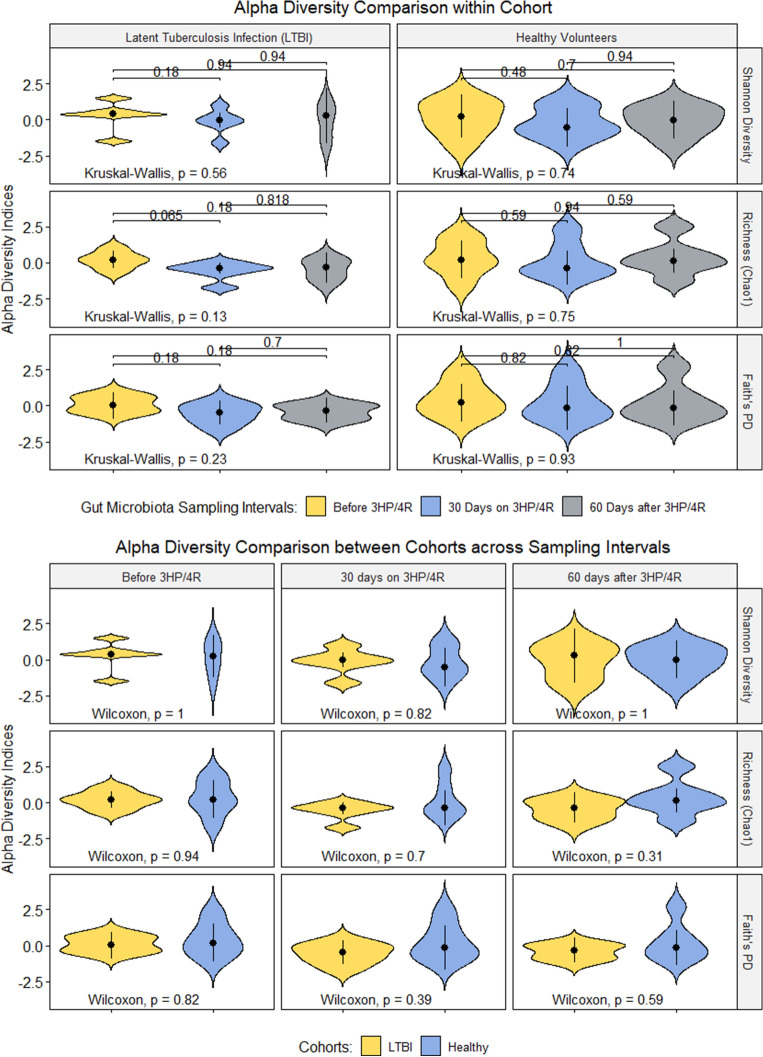
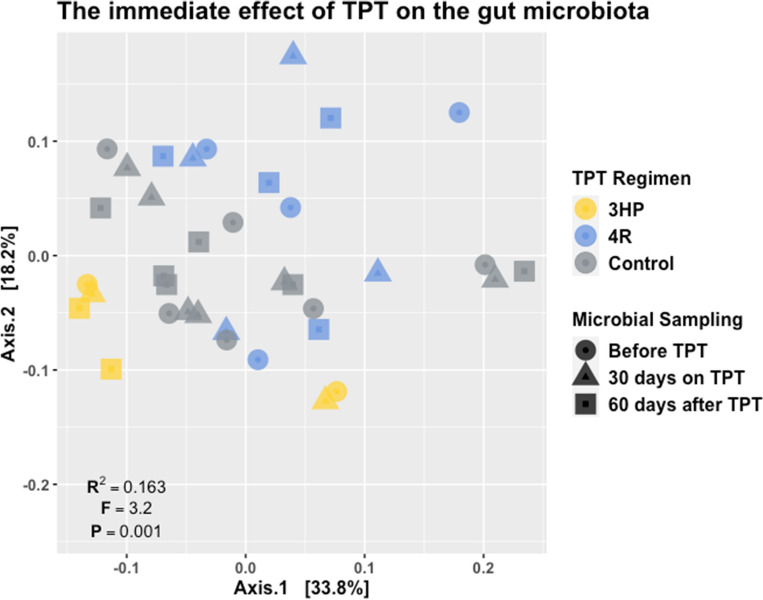
Tuberculosis (TB) preventive therapy (TPT) is an effective strategy to eliminate TB in low-incidence settings. Shorter TPT regimens incorporating the antimicrobial class of rifamycins are designed to improve adherence and completion rates but carry the risk of modifications to the gut microbiota. We enrolled six subjects diagnosed with latent TB infection (LTBI) who accepted to initiate TPT. We also enrolled six healthy volunteers unexposed to the rifamycins. We profiled the gut microbiota using 16S rRNA amplicon sequencing (V1-V2 region) to document the immediate effect of rifamycin-based TPT on the gut microbiota composition and tracked recovery to baseline two months after TPT. Overall, TPT accounted for 17% of the variance in gut microbial community dissimilarity. This rifamycin-based TPT induced dysbiosis was characterized by a depletion of butyrate-producing taxa (Clostridium-XIVa and Roseburia) and expansion of potentially pathogenic taxa within the Firmicutes and Proteobacteria phyla. Recovery of the gut microbial composition was incomplete two months after TPT. Robust clinical studies are necessary to comprehensively catalogue TPT-induced gut microbiota dysbiosis to inform strategies to mitigate potential long-term sequelae of this important TB control intervention.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
