

Whole brain network effects of subcallosal cingulate deep brain stimulation for treatment-resistant depression
- PMID: 37919403
- PMCID: PMC11078711
- DOI: 10.1038/s41380-023-02306-6
Whole brain network effects of subcallosal cingulate deep brain stimulation for treatment-resistant depression
Abstract
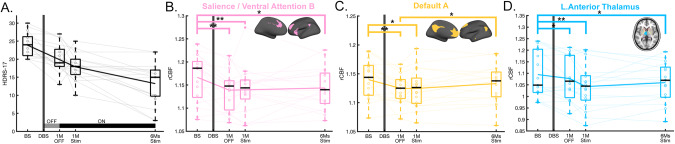
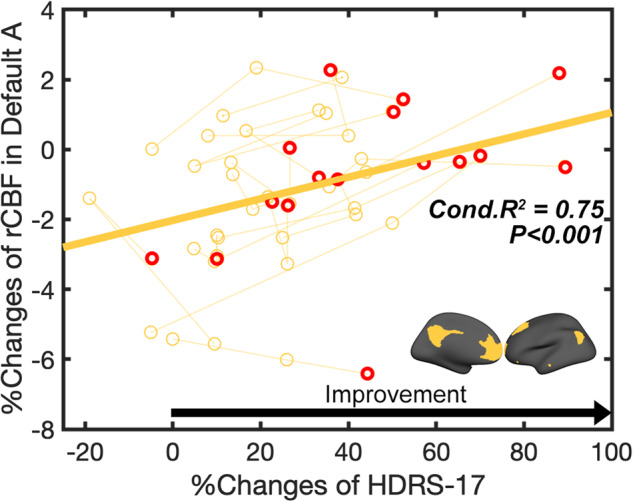
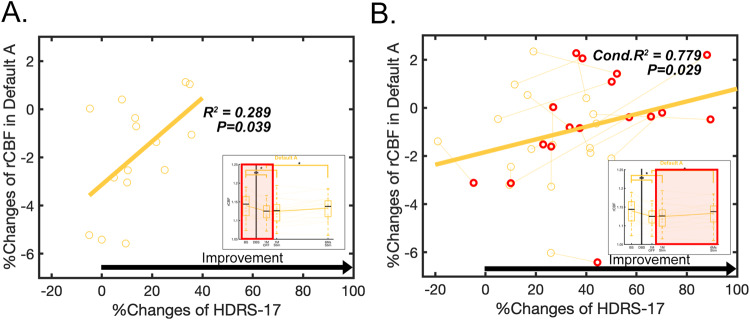
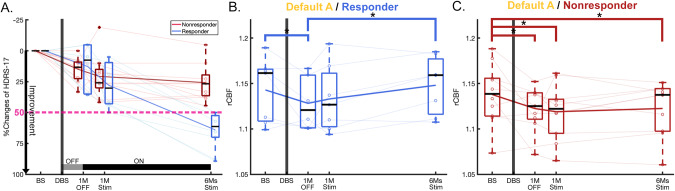
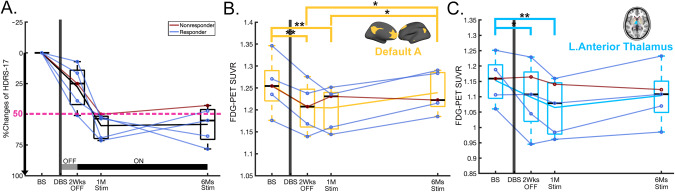
Ongoing experimental studies of subcallosal cingulate deep brain stimulation (SCC DBS) for treatment-resistant depression (TRD) show a differential timeline of behavioral effects with rapid changes after initial stimulation, and both early and delayed changes over the course of ongoing chronic stimulation. This study examined the longitudinal resting-state regional cerebral blood flow (rCBF) changes in intrinsic connectivity networks (ICNs) with SCC DBS for TRD over 6 months and repeated the same analysis by glucose metabolite changes in a new cohort. A total of twenty-two patients with TRD, 17 [15 O]-water and 5 [18 F]-fluorodeoxyglucose (FDG) positron emission tomography (PET) patients, received SCC DBS and were followed weekly for 7 months. PET scans were collected at 4-time points: baseline, 1-month after surgery, and 1 and 6 months of chronic stimulation. A linear mixed model was conducted to examine the differential trajectory of rCBF changes over time. Post-hoc tests were also examined to assess postoperative, early, and late ICN changes and response-specific effects. SCC DBS had significant time-specific effects in the salience network (SN) and the default mode network (DMN). The rCBF in SN and DMN was decreased after surgery, but responder and non-responders diverged thereafter, with a net increase in DMN activity in responders with chronic stimulation. Additionally, the rCBF in the DMN uniquely correlated with depression severity. The glucose metabolic changes in a second cohort show the same DMN changes. The trajectory of PET changes with SCC DBS is not linear, consistent with the chronology of therapeutic effects. These data provide novel evidence of both an acute reset and ongoing plastic effects in the DMN that may provide future biomarkers to track clinical improvement with ongoing treatment.
© 2023. The Author(s).
Conflict of interest statement
KC receives consulting fees from Abbott Neuromodulation. PRP receives consulting fees from Abbott Neuromodulation, LivaNova, Janssen Pharmaceuticals. PEH receives royalties from UpToDate and Oxford University Press. MF receives consulting fees from Medtronic. BHK receives consulting fees from Abbott Neuromodulation and Medtronic. HSM receives consulting and IP licensing fees from Abbott labs.
Figures
Update of
-
Whole Brain Network effects of subcallosal cingulate deep brain stimulation for treatment-resistant depression.Res Sq [Preprint]. 2023 Jun 14:rs.3.rs-3025802. doi: 10.21203/rs.3.rs-3025802/v1. Res Sq. 2023. Update in: Mol Psychiatry. 2024 Jan;29(1):112-120. doi: 10.1038/s41380-023-02306-6. PMID: 37398243 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
