

Single-cell analysis of immune recognition in chronic myeloid leukemia patients following tyrosine kinase inhibitor discontinuation
- PMID: 37919606
- PMCID: PMC10776410
- DOI: 10.1038/s41375-023-02074-w
Single-cell analysis of immune recognition in chronic myeloid leukemia patients following tyrosine kinase inhibitor discontinuation
Abstract
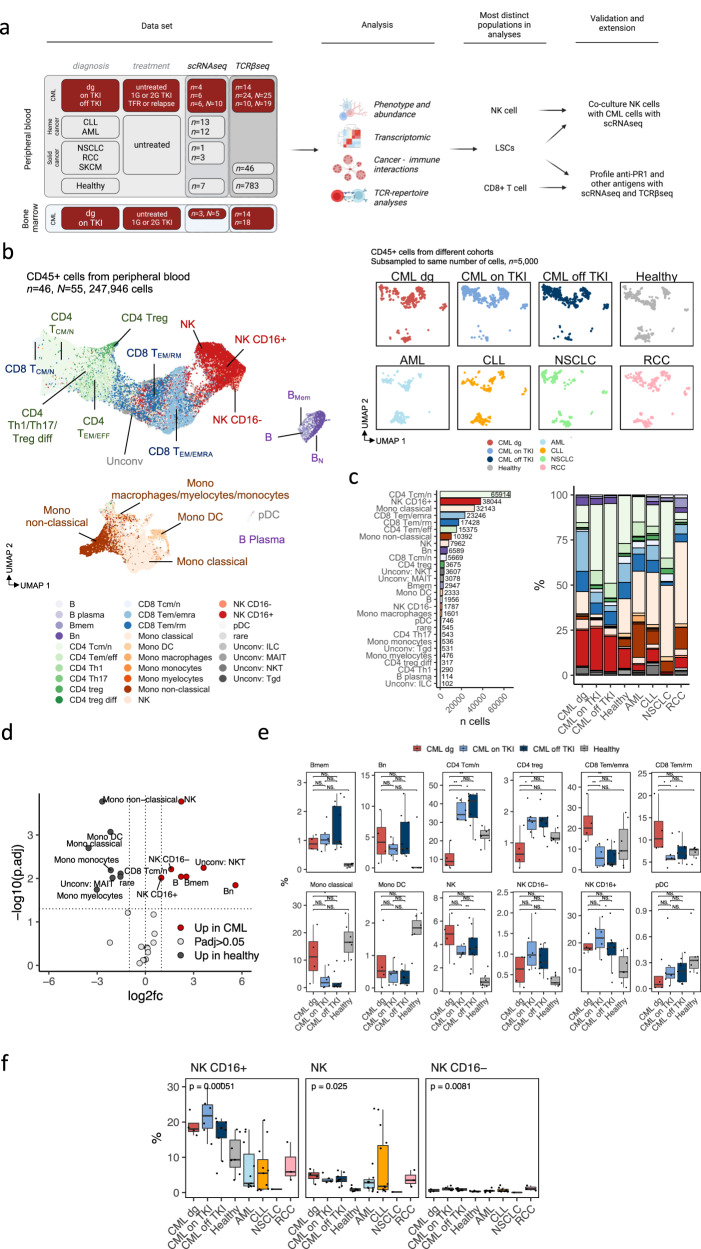
Immunological control of residual leukemia cells is thought to occur in patients with chronic myeloid leukemia (CML) that maintain treatment-free remission (TFR) following tyrosine kinase inhibitor (TKI) discontinuation. To study this, we analyzed 55 single-cell RNA and T cell receptor (TCR) sequenced samples (scRNA+TCRαβ-seq) from patients with CML (n = 13, N = 25), other cancers (n = 28), and healthy (n = 7). The high number and active phenotype of natural killer (NK) cells in CML separated them from healthy and other cancers. Most NK cells in CML belonged to the active CD56dim cluster with high expression of GZMA/B, PRF1, CCL3/4, and IFNG, with interactions with leukemic cells via inhibitory LGALS9-TIM3 and PVR-TIGIT interactions. Accordingly, upregulation of LGALS9 was observed in CML target cells and TIM3 in NK cells when co-cultured together. Additionally, we created a classifier to identify TCRs targeting leukemia-associated antigen PR1 and quantified anti-PR1 T cells in 90 CML and 786 healthy TCRβ-sequenced samples. Anti-PR1 T cells were more prevalent in CML, enriched in bone marrow samples, and enriched in the mature, cytotoxic CD8 + TEMRA cluster, especially in a patient maintaining TFR. Our results highlight the role of NK cells and anti-PR1 T cells in anti-leukemic immune responses in CML.
© 2023. The Author(s).
Conflict of interest statement
P.D. is currently employed by Nygen Analytics AB. M.I. is currently employed by Bristol Myers Squibb. U.O.S. has received honoraria from Incyte. H.H.H. has received honoraria from Novartis, Bristol Myers Squibb, and Incyte. A.B. has received honoraria from Novartis and MSD. G.K. is currently employed by Nygen Analytics AB. A.K. is currently employed by Bristol Myers Squibb. S.M. has received honoraria from Bristol Myers Squibb and DrenBio and research funding from BMS, Novartis, and Pfizer. All other authors declare no conflicts of interests.
Figures





References
-
- Mahon FX, Réa D, Guilhot J, Guilhot F, Huguet F, Nicolini F, et al. Discontinuation of imatinib in patients with chronic myeloid leukaemia who have maintained complete molecular remission for at least 2 years: the prospective, multicentre Stop Imatinib (STIM) trial. Lancet Oncol. 2010;11:1029–35. - PubMed
-
- Ross DM, Branford S, Seymour JF, Schwarer AP, Arthur C, Yeung DT, et al. Safety and efficacy of imatinib cessation for CML patients with stable undetectable minimal residual disease: results from the TWISTER study. Blood. 2013;122:515–22. - PubMed
-
- Saussele S, Richter J, Guilhot J, Gruber FX, Hjorth-Hansen H, Almeida A, et al. Discontinuation of tyrosine kinase inhibitor therapy in chronic myeloid leukaemia (EURO-SKI): a prespecified interim analysis of a prospective, multicentre, non-randomised, trial. Lancet Oncol. 2018;19:747–57. - PubMed
-
- Mori S, Vagge E, le Coutre P, Abruzzese E, Martino B, Pungolino E, et al. Age and dPCR can predict relapse in CML patients who discontinued imatinib: the ISAV study. Am J Hematol. 2015;90:910–4. - PubMed
-
- Nicolini FE, Dulucq S, Guilhot J, Etienne G, Mahon F-X. The Evaluation of Residual Disease By Digital PCR, and TKI Duration Are Critical Predictive Factors for Molecular Recurrence after for Stopping Imatinib First-Line in Chronic Phase CML Patients: Results of the STIM2 Study. Blood. 2018;132:462. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
