

Recent UK type 2 diabetes treatment guidance represents a near whole population indication for SGLT2-inhibitor therapy
- PMID: 37919773
- PMCID: PMC10623735
- DOI: 10.1186/s12933-023-02032-x
Recent UK type 2 diabetes treatment guidance represents a near whole population indication for SGLT2-inhibitor therapy
Abstract
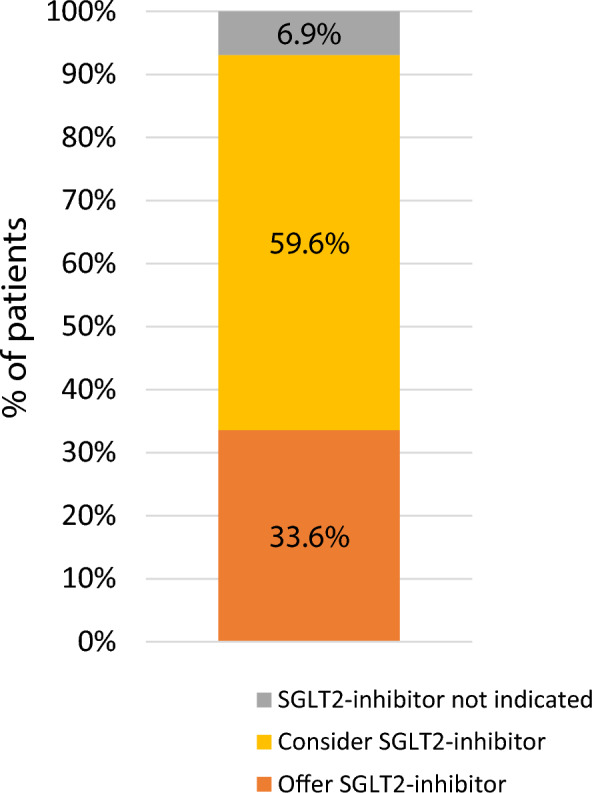
Recent type 2 diabetes guidance from the UK's National Institute for Health and Care Excellence (NICE) proposes offering SGLT2-inhibitor therapy to people with established atherosclerotic cardiovascular disease (ASCVD) or heart failure, and considering SGLT2-inhibitor therapy for those at high-risk of cardiovascular disease defined as a 10-year cardiovascular risk of > 10% using the QRISK2 algorithm. We used a contemporary population-representative UK cohort of people with type 2 diabetes to assess the implications of this guidance. 93.1% of people currently on anti-hyperglycaemic treatment are now recommended or considered for SGLT2-inhibitor therapy under the new guidance, with the majority (59.6%) eligible on the basis of QRISK2 rather than established ASCVD or heart failure (33.6%). Applying these results to the approximately 2.20 million people in England currently on anti-hyperglycaemic medication suggests 1.75 million people will now be considered for additional SGLT2-inhibitor therapy, taking the total cost of SGLT2-inhibitor therapy in England to over £1 billion per year. Given that older people, those of non-white ethnic groups, and those at lower cardiovascular disease risk were underrepresented in the clinical trials which were used to inform this guidance, careful evaluation of the impact and safety of increased SGLT2-inhibitor prescribing across different populations is urgently required. Evidence of benefit should be weighed against the major cost implications for the UK National Health Service.
Keywords: Cardiovascular disease; Diabetes mellitus type 2; SGLT2-inhibitors.
© 2023. The Author(s).
Conflict of interest statement
APM declares previous research funding from Pfizer and Boehringer-Ingelheim outside the submitted work. All other authors declare no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- National Institute for Health and Care Excellence (NICE). Type 2 diabetes in adults: management NICE guideline (NG28). https://www.nice.org.uk/guidance/ng28. Accessed 15 Mar 2022. - PubMed
-
- National Institute for Health and Care Excellence (NICE). Type 2 diabetes [B] Pharmacological therapies with cardiovascular and other benefits in people with type 2 diabetes. https://www.nice.org.uk/Guidance/NG28/evidence. Accessed 15 Mar 2022. - PubMed
-
- Openprescribing. Prescription data for Canagliflozin, Dapagliflozin, and Empagliflozin. 2020. https://openprescribing.net/. Accessed 15 Mar 2022.
-
- NHS Digital. Prescriptions dispensed in the community—statistics for england, 2007–2017. 2018. https://digital.nhs.uk/data-and-information/publications/statistical/pre.... Accessed 15 Mar 2022.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
