

Recruitment of pre-dementia participants: main enrollment barriers in a longitudinal amyloid-PET study
- PMID: 37919783
- PMCID: PMC10621165
- DOI: 10.1186/s13195-023-01332-4
Recruitment of pre-dementia participants: main enrollment barriers in a longitudinal amyloid-PET study
Abstract
Background: The mismatch between the limited availability versus the high demand of participants who are in the pre-dementia phase of Alzheimer's disease (AD) is a bottleneck for clinical studies in AD. Nevertheless, potential enrollment barriers in the pre-dementia population are relatively under-reported. In a large European longitudinal biomarker study (the AMYPAD-PNHS), we investigated main enrollment barriers in individuals with no or mild symptoms recruited from research and clinical parent cohorts (PCs) of ongoing observational studies.
Methods: Logistic regression was used to predict study refusal based on sex, age, education, global cognition (MMSE), family history of dementia, and number of prior study visits. Study refusal rates and categorized enrollment barriers were compared between PCs using chi-squared tests.
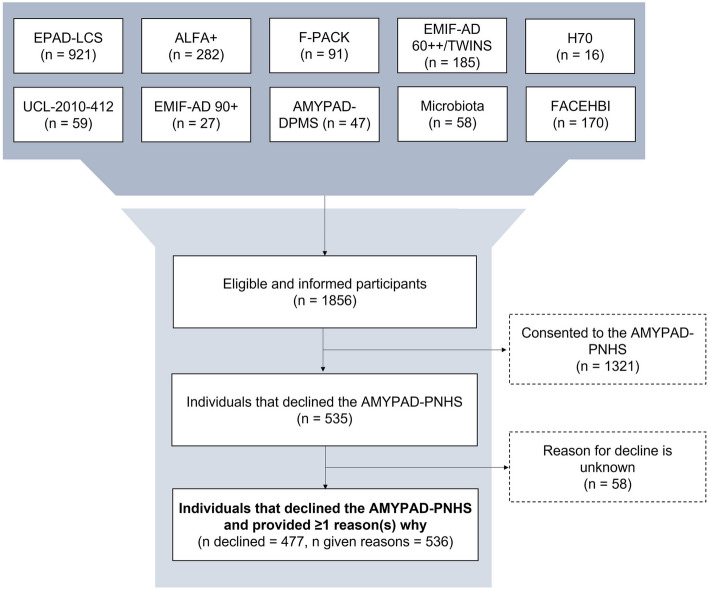
Results: 535/1856 (28.8%) of the participants recruited from ongoing studies declined participation in the AMYPAD-PNHS. Only for participants recruited from clinical PCs (n = 243), a higher MMSE-score (β = - 0.22, OR = 0.80, p < .05), more prior study visits (β = - 0.93, OR = 0.40, p < .001), and positive family history of dementia (β = 2.08, OR = 8.02, p < .01) resulted in lower odds on study refusal. General study burden was the main enrollment barrier (36.1%), followed by amyloid-PET related burden (PCresearch = 27.4%, PCclinical = 9.0%, X2 = 10.56, p = .001), and loss of research interest (PCclinical = 46.3%, PCresearch = 16.5%, X2 = 32.34, p < .001).
Conclusions: The enrollment rate for the AMYPAD-PNHS was relatively high, suggesting an advantage of recruitment via ongoing studies. In this observational cohort, study burden reduction and tailored strategies may potentially improve participant enrollment into trial readiness cohorts such as for phase-3 early anti-amyloid intervention trials. The AMYPAD-PNHS (EudraCT: 2018-002277-22) was approved by the ethical review board of the VU Medical Center (VUmc) as the Sponsor site and in every affiliated site.
Keywords: Alzheimer’s disease; Amyloid PET; Clinical trial; Enrollment barriers; Preclinical; Recruitment.
© 2023. The Author(s).
Conflict of interest statement
MB has been a consultant for Araclon, Avid, Bayer, Elan, Grifols, Janssen/Pfizer, Lilly, Neuroptix, Nutricia, Roche, Sanofi, Biogen, and Servier; and received fees for lectures and funds for research from Araclon, Esteve, Grifols, Janssen, Novartis, Nutricia, Piramal, Pfizer-Wyett, Roche, and Servier. Mercè Boada received research funding from the Instituto de Salud Carlos III (ISCIII) Acción Estratégica en Salud, integrated in the Spanish National RCDCI Plan and financed by ISCIII-Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER-Una manera de hacer Europa) grant PI17/01474, and the European Union/EFPIA Innovative Medicines Initiative Joint MOPEAD project (grant number 115985). MM received research funding from the Instituto de Salud Carlos III (ISCIII) Acción Estratégica en Salud, integrated in the Spanish National RCDCI Plan and financed by ISCIII-Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER-Una manera de hacer Europa) grant PI19/00335. DA received funding by the Fondation Recherche Alzheimer, and the Swiss National Science Foundation (project CRSK-3_196354 / 1). PS is a full-time employee of EQT Life Sciences (formerly LSP) and Professor Emeritus at Amsterdam University Medical Centers. Within his university affiliation he is global PI of the phase 1b study of AC Immune, Phase 2b study with FUJI-film/Toyama and phase 2 study of UCB. He is past chair of the EU steering committee of the phase 2b program of Vivoryon and the phase 2b study of Novartis Cardiology. Presently he co-chairs the phase 3 study with NOVO-Nordisk. RV his institution has Clinical Trial Agreements (as PI) with Alector, Biogen, Janssen Pharmaceuticals, NovoNordisk, Prevail, Roche, UCB. His institution has consultancy agreements (RV as DSMB member) with AC Immune and Novartis. PS has an editorial role for the Alzheimer’s Research & Therapy (AZRT) journal. RV was global PI of the Phase 1 and 2 18F-flutemetamol trials. RV institution had a material transfer agreement (RV as PI) with GEHC for free tracer delivery of the FPACK cohort baseline scans and with Avid Pharmaceuticals, an EliLilly subsidiary. BH received consulting fees from Biogen and Roche. The Belgian Foundation for Scientific Research supports his salary (FNRS CCL grant #40010417). He has received grants from the FNRS (including the WELBIO fund ##40010035), the Belgian Alzheimer Research Foundation (SAO-FRA), the Louvain and Saint-Luc Foundations, and the Queen Elizabeth Medical Foundation (QEMF-FMRE). MS has received fees for contributions to Advisory Boards from Roche, NovoNordisk and Servier and has received research support by Roche. MS has an editorial role for the AZRT journal. GBF reports grants from Avid Radiopharmaceuticals, Biogen, GE International, Guerbert, IXICO, Merz Pharma, Nestlé, Novartis, Eisai, Piramal, Roche, Siemens, Teva Pharmaceutical Industries, and Vifor Pharma; he has received personal fees from AstraZeneca, Avid Radiopharmaceuticals, Biogen, Roche, Diadem, Neurodiem, Elan Pharmaceuticals, GE International, Lundbeck, Pfizer, and TauRx Therapeutics. FJ reported receiving personal fees from Biogen, personal fees from Eisai, personal fees from Roche, personal fees from AC Immune, personal fees from Janssen, personal fees from Danone/Nutricia, personal fees from Lilly, personal fees from Grifols, and personal fees from Novo Nordisk outside the submitted work. FJ has an editorial role for the AZRT journal. AN received consulting fees from Hoffman La Roche. Patent: US patent alpha 7 nicotinic PET tracer. She is deputy chairman of Wennergren Foundations. MK has an editorial role for the AZRT journal. CWG has received fees for contributions to Advisory Boards from Biogen, Eisai, Eli Lilly, Roche, Roche Diagnostics, Actinogen, Alchemab, Merck, Kyowa Kirin, and Signant. His research has been supported by Janssen and Biogen. He was Chief Investigator of the IMI Funded EPAD project that had multiple EFPIA and SME partners. OG-R receives research support from Hoffmann La-Roche (paid to institution). JLM reported receiving grants from Innovative Medicines Initiative AMYPAD during the conduct of the study; being employed by Lundbeck and receiving consultancy fees from Genentech, Novartis, Oryzon, Biogen, Lilly, Janssen, Green Valley, MSD, Eisai, ProMIS Neurosciences, and Alector outside the submitted work. MS and LF are employees of Janssen Pharmaceuticals. AS and RG are employees of Life Molecular Imaging GmbH. JDG reported receiving grants from GE Healthcare, grants and personal fees from Roche Diagnostics, grants from Hoffmann La-Roche, personal fees from Biogen, and personal fees from Philips Nederland outside the submitted work. GF received research support from GE Healthcare (paid to institution). FB is in the steering committee or iDMC member for Biogen, Merck, Roche, EISAI and Prothena. Consultant for Roche, Biogen, Merck, IXICO, Jansen, Combinostics, FB h
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
