

Diagnostic, prognostic and clinical value of left ventricular radial strain to identify paradoxical septal motion in ventilated patients with the acute respiratory distress syndrome: an observational prospective multicenter study
- PMID: 37919787
- PMCID: PMC10623720
- DOI: 10.1186/s13054-023-04716-y
Diagnostic, prognostic and clinical value of left ventricular radial strain to identify paradoxical septal motion in ventilated patients with the acute respiratory distress syndrome: an observational prospective multicenter study
Abstract
Background: Acute cor pulmonale (ACP) is prognostic in patients with acute respiratory distress syndrome (ARDS). Identification of paradoxical septal motion (PSM) using two-dimensional echocardiography is highly subjective. We sought to describe feature-engineered metrics derived from LV radial strain changes related to PSM in ARDS patients with ACP of various severity and to illustrate potential diagnostic and prognostic yield.
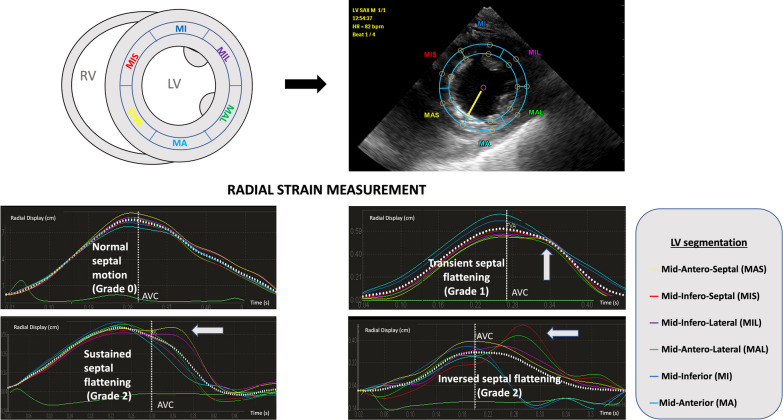
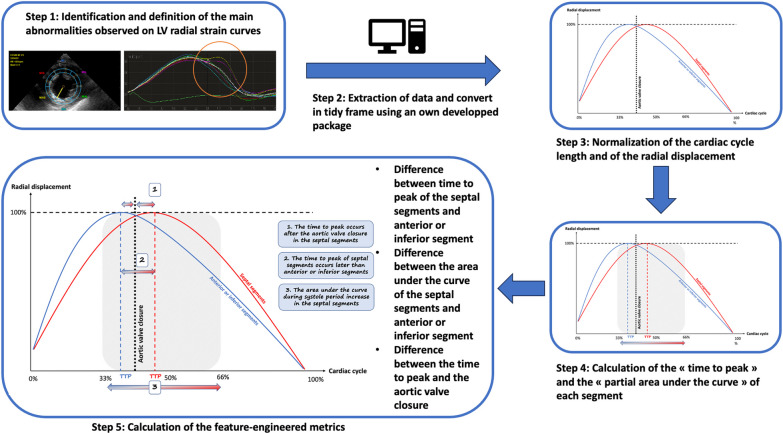
Methods: This prospective bicentric study included patients under protective ventilation for ARDS related to COVID-19 who were assessed using transesophageal echocardiography (TEE). Transgastric short-axis view at mid-papillary level was used to visually grade septal motion, using two-dimensional imaging, solely and combined with LV radial strain: normal (grade 0), transient end-systolic septal flattening (grade 1), prolonged end-systolic septal flattening or reversed septal curvature (grade 2). Inter-observer variability was calculated. Feature engineering was performed to calculate the time-to-peak and area under the strain curve in 6 LV segments. In the subset of patients with serial TEE examinations, a multivariate Cox model analysis accounting for new-onset of PSM as a time-dependent variable was used to identify parameters associated with ICU mortality.
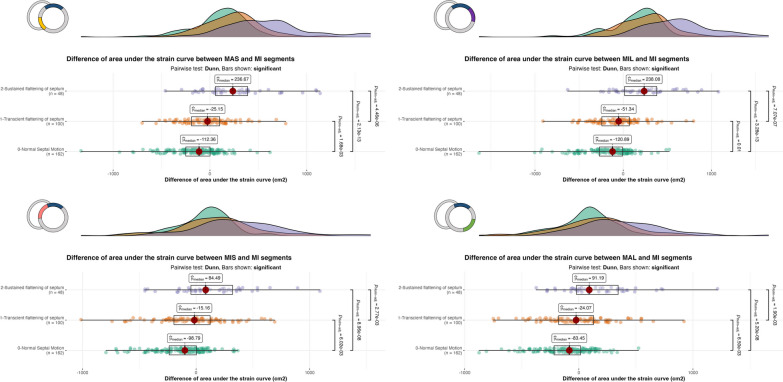
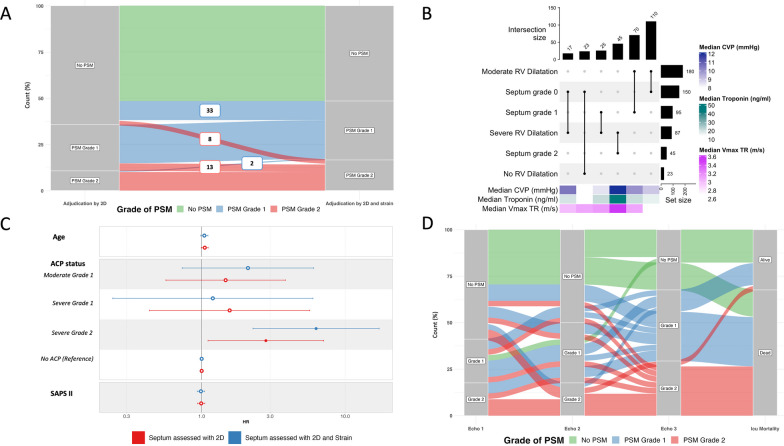
Results: Overall, 310 TEE examinations performed in 182 patients were analyzed (age: 67 [60-72] years; men: 66%; SAPSII: 35 [29-40]). Two-dimensional assessment identified a grade 1 and grade 2 PSM in 100 (32%) and 48 (15%) examinations, respectively. Inter-rater reliability was weak using two-dimensional imaging alone (kappa = 0.49; 95% CI 0.40-0.58; p < 0.001) and increased with associated LV radial strain (kappa = 0.84, 95% CI 0.79-0.90, p < 0.001). The time-to-peak of mid-septal and mid-lateral segments occurred significantly later in systole and increased with the grade of PSM. Similarly, the area under the strain curve of these segments increased significantly with the grade of PSM, compared with mid-anterior or mid-inferior segments. Severe acute cor pulmonale with a grade 2 PSM was significantly associated with mortality. Requalification in an upper PSM grade using LV radial strain allowed to better identify patients at risk of death (HR: 6.27 [95% CI 2.28-17.2] vs. 2.80 [95% CI 1.11-7.09]).
Conclusions: In objectively depicting PSM and quantitatively assessing its severity, TEE LV radial strain appears as a valuable adjunct to conventional two-dimensional imaging.
Keywords: Critical care; Pulmonary heart disease; Respiratory distress syndrome; Transesophageal echocardiography.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Sato R, Dugar S, Cheungpasitporn W, Schleicher M, Collier P, Vallabhajosyula S, et al. The impact of right ventricular injury on the mortality in patients with acute respiratory distress syndrome: a systematic review and meta-analysis. Crit Care. 2021;25:172. doi: 10.1186/s13054-021-03591-9. - DOI - PMC - PubMed
-
- Evrard B, Goudelin M, Giraudeau B, François B, Vignon P. Right ventricular failure is strongly associated with mortality in patients with moderate-to-severe COVID-19-related ARDS and appears related to respiratory worsening. Intensive Care Med. 2022;48:765–767. doi: 10.1007/s00134-022-06730-0. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
