

Mycosis fungoides with spongiosis: a case report
- PMID: 37919795
- PMCID: PMC10623773
- DOI: 10.1186/s13256-023-04188-2
Mycosis fungoides with spongiosis: a case report
Abstract
Background: Mycosis fungoides (MF) is the most common form of cutaneous T-cell lymphoma (CTCL). CTCL are an uncommon, heterogeneous group of non-Hodgkin lymphomas (NHLs) of T- and B-cell origin where the skin is the primary organ of involvement. It is characterized by malignant CD4+ T-cells infiltrating the skin and other organs, leading to progressive skin and systemic involvement. Histopathologically, MF is characterized by atypical lymphocytes demonstrating epidermotropism without spongiosis. Spongiosis is the histological hallmark of intercellular epidermal edema, viewed as clear spaces within the epidermis, and is very common in benign inflammatory dermatoses. Very few studies have reported MF in sub-Saharan Africa (SSA). We are reporting a case of MF with a rare presentation of spongiosis treated successfully with a low dose total skin electron beam therapy (TSEBT) followed by maintenance therapy of low dose Methotrexate (MT) at the Ocean Road Cancer Institute (ORCI) in Tanzania. This is the first case of MF to be managed with low-dose TSEBT in Tanzania. The authors wish to create awareness of the disease among physicians and pathologists and expand on the data paucity in SSA.
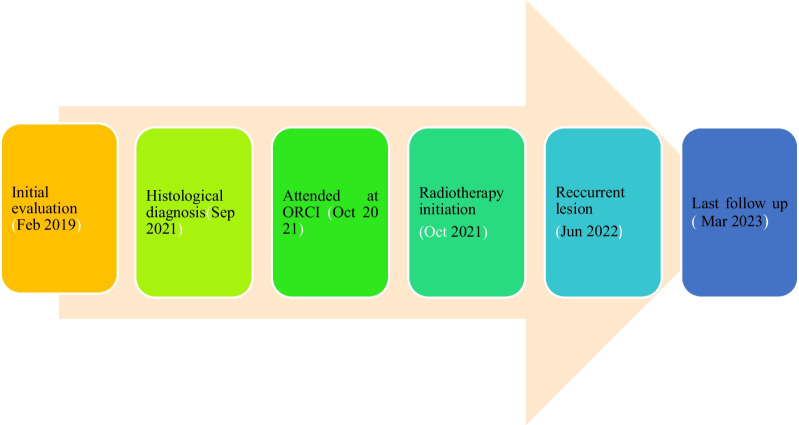
Case description: We are reporting a case of a 31-year-old male of African origin who self-referred to our oncology center with a 4-year history of skin rashes throughout the body, which was unresponsive to topical steroid treatment. The biopsy was taken, and the patient was diagnosed with MF CD 3 positive with spongiosis. The patient was treated with radiotherapy, whereby he received low dose total skin electron beam therapy (TSEBT) 12 Gy in 3 fractions at a daily dose of 4 Gy, followed by maintenance therapy of low dose Methotrexate and attained an excellent therapeutic response.
Conclusion: Spongiosis is an infrequent presentation of MF. Low-dose TSEBT provides reliable and rapid reduction of disease burden in patients with MF, which could be administered safely multiple times during a patient's disease with an acceptable toxicity profile. Lack of tendency to perform skin biopsies and cost constraints in assessing multiple immunophenotypic markers lead to missing the diagnosis. Diagnosis and treatment of MF in resource-limited countries is challenging.
Keywords: Case report; Chemotherapy; Mycosis fungoides; Ocean Road Cancer Institute; Total skin electron beam radiotherapy.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors do not disclose any conflict of interest.
Figures








References
-
- Jean L. Bolognia, Julie V. Schaffer LC. Dermatology: 2-Volume Set, 4th Edition. 4th ed. elsevier health, editor. Elsevier; 2017. chap 131.
-
- Yamashita T, Fernandes Abbade LP, Esther M, Marques A, Marques SA, Pathology I. CONTINUED MEDICAL EDUCATION Mycosis fungoides and Sézary syndrome: clinical, histopathological and immunohistochemical review and update Work conducted at the. An Bras Dermatol. 2012;87(6):817–847. doi: 10.1590/S0365-05962012000600001. - DOI - PMC - PubMed
-
- Quaglino P, Maule M, Prince HM, Porcu P, Horwitz S, Duvic M, et al. Global patterns of care in advanced stage mycosis fungoides/Sezary syndrome: a multicenter retrospective follow-up study from the Cutaneous Lymphoma International Consortium. Ann Oncol. 2017;28(10):2517–2525. doi: 10.1093/annonc/mdx352. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
