

Multimodal diagnostics for keratoconus and ectatic corneal diseases: a paradigm shift
- PMID: 37919821
- PMCID: PMC10623885
- DOI: 10.1186/s40662-023-00363-0
Multimodal diagnostics for keratoconus and ectatic corneal diseases: a paradigm shift
Abstract
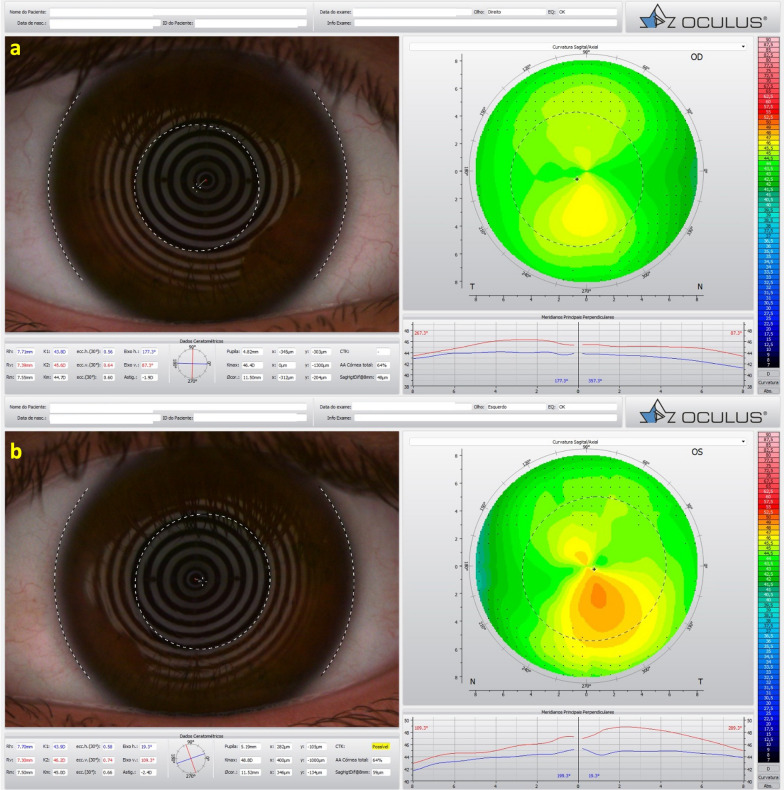
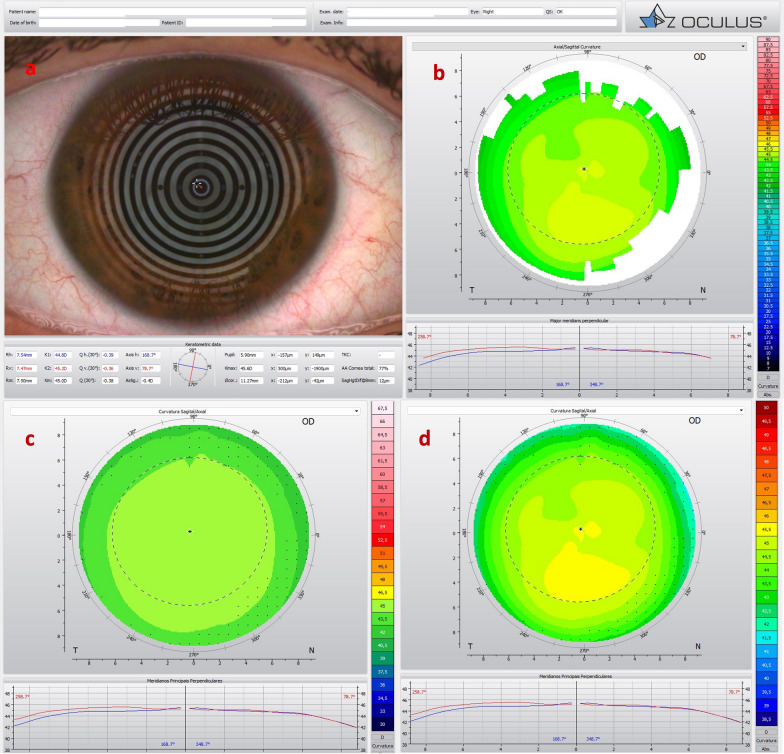
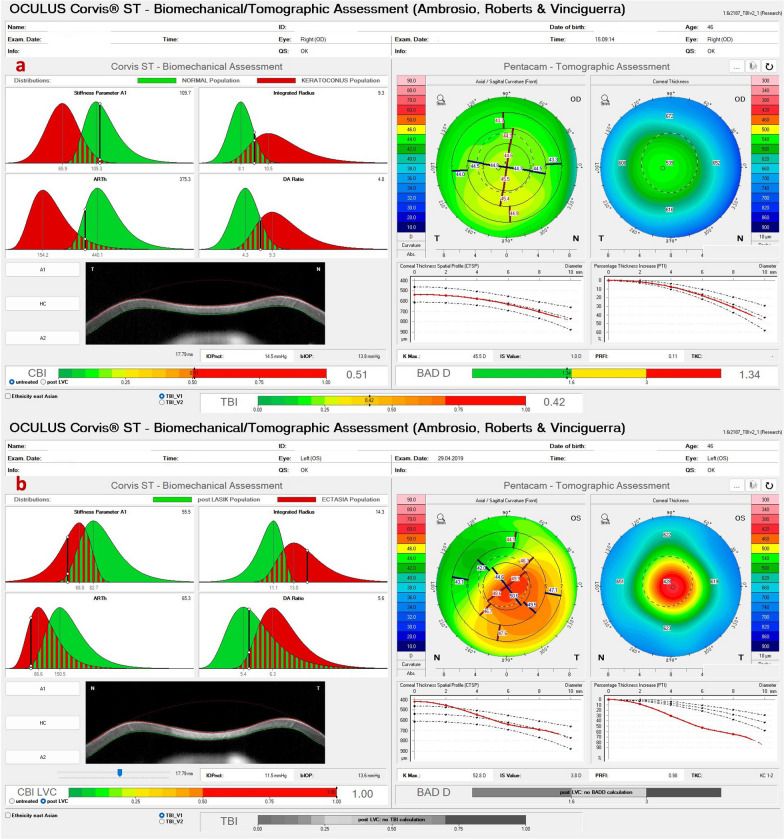
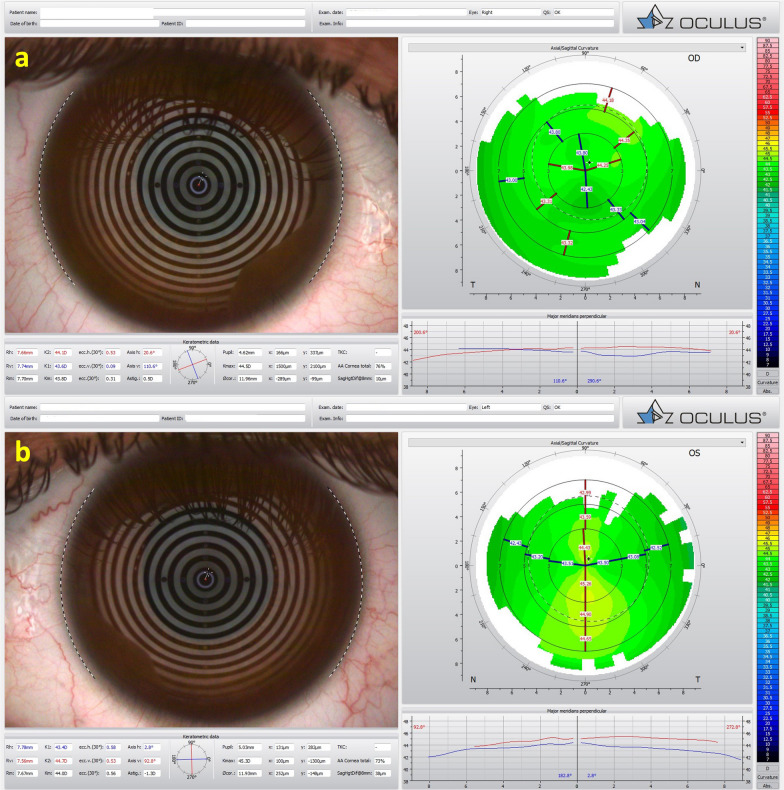
Different diagnostic approaches for ectatic corneal diseases (ECD) include screening, diagnosis confirmation, classification of the ECD type, severity staging, prognostic evaluation, and clinical follow-up. The comprehensive assessment must start with a directed clinical history. However, multimodal imaging tools, including Placido-disk topography, Scheimpflug three-dimensional (3D) tomography, corneal biomechanical evaluations, and layered (or segmental) tomography with epithelial thickness by optical coherence tomography (OCT), or digital very high-frequency ultrasound (dVHF-US) serve as fundamental complementary exams for measuring different characteristics of the cornea. Also, ocular wavefront analysis, axial length measurements, corneal specular or confocal microscopy, and genetic or molecular biology tests are relevant for clinical decisions. Artificial intelligence enhances interpretation and enables combining such a plethora of data, boosting accuracy and facilitating clinical decisions. The applications of diagnostic information for individualized treatments became relevant concerning the therapeutic refractive procedures that emerged as alternatives to keratoplasty. The first paradigm shift concerns the surgical management of patients with ECD with different techniques, such as crosslinking and intrastromal corneal ring segments. A second paradigm shift involved the quest for identifying patients at higher risk of progressive iatrogenic ectasia after elective refractive corrections on the cornea. Beyond augmenting the sensitivity to detect very mild (subclinical or fruste) forms of ECD, ectasia risk assessment evolved to characterize the inherent susceptibility for ectasia development and progression. Furthermore, ectasia risk is also related to environmental factors, including eye rubbing and the relational impact of the surgical procedure on the cornea.
Keywords: Corneal biomechanics; Corneal ectasia; Corneal tomography; Keratoconus; Multimodal corneal imaging; Refractive surgery; Susceptibility.
© 2023. The Author(s).
Conflict of interest statement
Dr. Ambrósio is a consultant for Oculus, Alcon, Zeiss and Mediphacos.
Figures







References
-
- Ambrósio R, Jr, Lopes B, Amaral J, Faria-Correia F, Canedo ALC, Salomão MQ, et al. Keratoconus: breaking paradigms and contradictions of a new subspecialty. Rev Bras Oftalmol. 2019;78(2):81–85.
-
- Ambrósio R., Jr Cirurgia refrativa terapêutica: por que diferenciar? Rev Bras Oftalmol. 2013;72(2):85–86. doi: 10.1590/S0034-72802013000200002. - DOI
Publication types
LinkOut - more resources
Full Text Sources
