

Early Oral Antibiotic Switch in Staphylococcus aureus Bacteraemia: The Staphylococcus aureus Network Adaptive Platform (SNAP) Trial Early Oral Switch Protocol
- PMID: 37921609
- PMCID: PMC11478773
- DOI: 10.1093/cid/ciad666
Early Oral Antibiotic Switch in Staphylococcus aureus Bacteraemia: The Staphylococcus aureus Network Adaptive Platform (SNAP) Trial Early Oral Switch Protocol
Abstract
Background: Staphylococcus aureus bloodstream infection (bacteremia) is traditionally treated with at least 2 weeks of intravenous (IV) antibiotics in adults, 3-7 days in children, and often longer for those with complicated disease. The current practice of treating S. aureus bacteremia (SAB) with prolonged IV antibiotics (rather than oral antibiotics) is based on historical observational research and expert opinion. Prolonged IV antibiotic therapy has significant disadvantages for patients and healthcare systems, and there is growing interest in whether a switch to oral antibiotics following an initial period of IV therapy is a safe alternative for clinically stable patients.
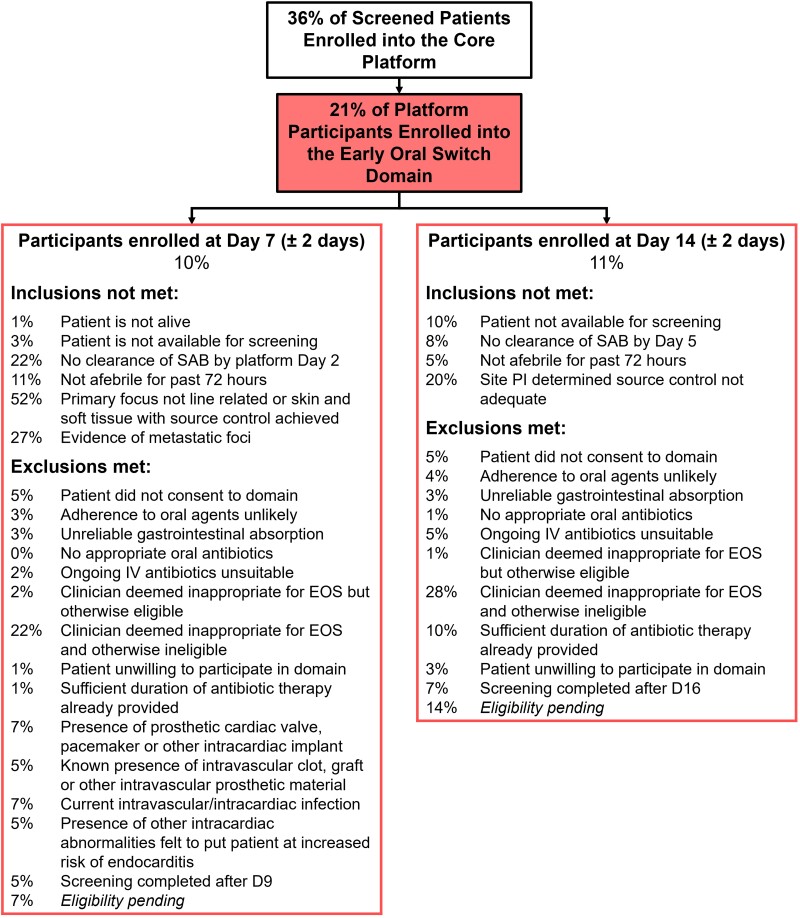
Protocol: The early oral switch (EOS) domain of the S. aureus Network Adaptive Platform (SNAP) trial will assess early switch to oral antibiotics compared with continued IV treatment in clinically stable patients with SAB. The primary endpoint is 90-day all-cause mortality. Hospitalised SAB patients are assessed at platform day 7 ±2 (uncomplicated SAB) and day 14 ±2 (complicated SAB) to determine their eligibility for randomization to EOS (intervention) or continued IV treatment (current standard of care).
Discussion: Recruitment is occurring in the EOS domain of the SNAP trial. As of August 2023, 21% of all SNAP participants had been randomized to the EOS domain, a total of 264 participants across 77 centers, with an aim to recruit at least 1000 participants. We describe challenges and facilitators to enrolment in this domain to aid those planning similar trials.
Trial registration: ClinicalTrials.gov NCT05137119.
Keywords: Staphylococcus aureus (or S. aureus); adaptive platform clinical trial; bacteremia (or bacteraemia or bloodstream infection); intravenous antibiotic; oral antibiotic.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. A. McGlothlin is an employee of Berry Consultants, LLC, a statistical consulting firm that specializes in the design of adaptive and platform clinical trials. Berry Consultants received compensation for work included in the content of the submission. A. C. Bowen reports participation as a member of the CAMERA-2 data and safety monitoring board (DSMB) and as chair of the Skin Trial DSMB; she also reports participation on Phage Trial DSMB and participation as Chair of FOSUTI DSMB; a role as Vice President of the World Society of Paediatric Infectious Diseases and as Co-Chair, Australian and New Zealand Pediatric Infectious Diseases group of the Australasian Society of Infectious Diseases (ASID). D. L. Paterson reports grants or contracts made to institution and unrelated to this work from Shionogi, Merck, and Pfizer; consulting fees to author from Antimicrobial Resistance Action Fund and Spero Therapeutics; payment or honoraria for lectures, presentations, speaker's bureaus, manuscript writing, or educational events to author from Pfizer and Merck; support for attending meetings and/or travel to author from Pfizer; and an unpaid leadership or fiduciary role with ASID. J. A. Roberts reports contracts or grants paid to institution and unrelated to this work from Pfizer and QPEX and investigator grant (APP2009736) and Advancing Queensland Clinical Fellowship; consulting fees paid to author from QPEX, Advanz Pharma, Gilead, Pfizer, Sandoz, Summit Pharma, and MSD; payment to author for lectures, presentations, speaker's bureaus, manuscript writing, or educational events from MSD, Gilead, Pfizer, and Cipla. J. Ten Oever reports grants or contracts unrelated to this work from Pfizer and MSD; support for attending meetings and/or travel to author from Pfizer; M. P. Cheng reports research support from the Canadian Institutes of Health Research and is supported by the Fonds de Recherche du Québec—Santé; research contracts from Cidara Therapeutics, Scynexis, and Amplyx Pharmaceuticals; consulting fees as a scientific consultant for AstraZeneca, Takeda, Merck, and Pfizer; 3 pending patents (Methods for detecting tissue damage, graft-versus-host disease, and infections using cell-free DNA profiling; Methods for assessing the severity and progression of SARS-CoV-2 infections using cell-free DNA; and rapid identification of antimicrobial resistance and other microbial phenotypes using highly multiplexed fluorescence in situ hybridization); stock options as a member of the scientific advisory board for GEn1E Lifesciences and Nomic Bio; and equity as co-founder of Kanvas Biosciences. R. J. Lewis is an employee of Berry Consultants, LLC, a statistical consulting firm that specializes in the design of adaptive and platform clinical trials. Berry Consultants received compensation for work included in the content of the submission. S. A. W. reports personal consulting fees from ClinicIQ pharma and Roche; an unpaid role as chair of Australian Clinical Trials Alliance; and stock and options with ClinicIQ. S. C. Morpeth reports grants or contracts unrelated to this work from the HRC, and a nonremunerated role as the Chair of the New Zealand Microbiology Network. S. Kalimuddin reports consulting fees from Gilead, Janssen, and Takeda (payments made to Singapore General Hospital) and grants or contracts unrelated to this work from National Medical Research Council, Singapore. S. Y. C. Tong reports a contract as a paid consultant for advice on clinical trial design, and consulting fees from Roivant Sciences as a paid consultant for advice on clinical trial design; and reports grants or contracts unrelated to this work from Australian National Health and Medical Research Council. T. C. Lee reports research salary support from Fonds de Recherche Quebec–Sante, operating funds for other studies including CATCO from the CIHR; and operating funds for other studies from the McGill Interdisciplinary Institute Infection and Immunity. Conflicts that the editors consider relevant to the content of the article have been disclosed. Collaborating authors have not been asked for their potential conflicts. A. Campbell reports National Health and Medical Research Council (grant 2014900) for SNAPPY and Perth Children's Hospital Foundation for site funding for SNAPPY and Raine Clinician Fellowship; participation on Data safety monitoring board for the B part of the NT Meningococcal B study; a role as Co-chair Australian and New Zealand Pediatric Infectious Diseases Special Interest Group Committee. A. Legg reports payment to author for Australian Pharmacy Council—EVUSHELD module and webinar and SHPA webinar; support for attending meetings and/or travel from Therapeutic Guidelines group meeting. L. Whiteway reports being remunerated for time attending meetings, and review of patient facing materials as consumer/PPI representative on the SNAP global trial steering committee. M. Bonten reports grants or contracts (all payments to UMCU) from Janssen Vaccines, Merck, LimmaTech, CureVac, Spherecydes; consulting fees (all payments to UMCU) from Janssen Vaccines, AstraZeneca, Pfizer, Sperecydes, Shionogi, GSK; participation on Data Safety Monitoring Board or Advisory Board for Sanofi (payments to UMCU). S. A. Webb reports grant from National Health and Medical Research Council of Australia that supports SNAP; personal consultings fees from ClinicIQ pharma and Roche; no patents or participation on Data Safety Monitoring Boards or Advisory Boards relevant to this work; unpaid roles as Chair and Director of Australian Clinical Trials Alliance; stock or stock options with Reliis. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis 2011; 52:e18–55. - PubMed
-
- Broom J, Broom A, Adams K, Plage S. What prevents the intravenous to oral antibiotic switch? A qualitative study of hospital doctors’ accounts of what influences their clinical practice. J Antimicrob Chemother 2016; 71:2295–9. - PubMed
-
- Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC guidelines for the management of infective endocarditis. Eur Heart J 2015; 36:3075–128. - PubMed
-
- Campbell AJ, Al Yazidi LS, Phuong LK, et al. Pediatric Staphylococcus aureus bacteremia: clinical spectrum and predictors of poor outcome. Clin Infect Dis 2022; 74:604–13. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
