

CCTA-based CABG SYNTAX Score: a tool to evaluate completeness of coronary segment revascularization after bypass surgery
- PMID: 37921898
- PMCID: PMC10692266
- DOI: 10.1007/s10554-023-02978-9
CCTA-based CABG SYNTAX Score: a tool to evaluate completeness of coronary segment revascularization after bypass surgery
Abstract
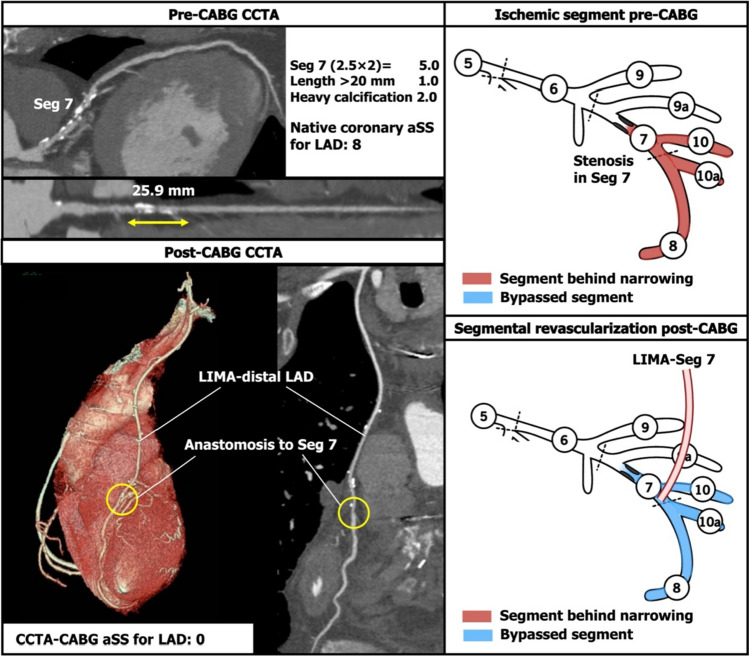
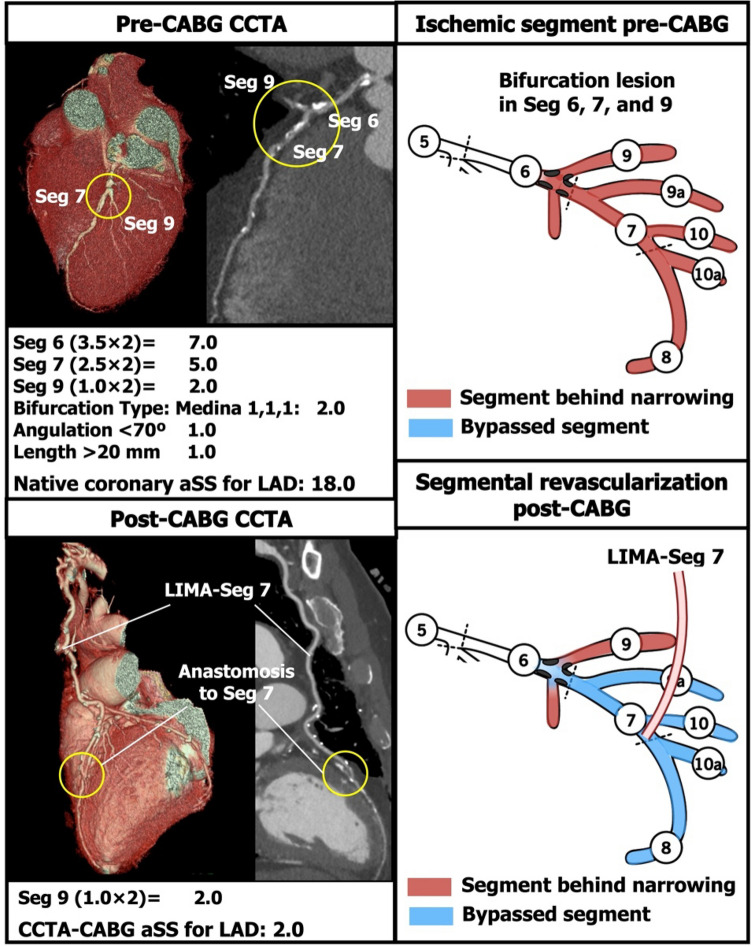
To describe the updated coronary computed tomographic angiography (CCTA)-based coronary artery bypass graft (CABG) anatomic SYNTAX Score (aSS) and assess its utility and reproducibility for assessing the completeness of revascularization after CABG. The CCTA-CABG aSS is a visual assessment using CCTA post-CABG which quantifies the failure in effectively grafting stenotic coronary segments, and therefore assesses the completeness of surgical revascularization. It is calculated by subtracting the aSS of successfully anastomosed coronary segments from the aSS of the native coronary tree. The inter-observer reproducibility of the CCTA-CABG aSS was evaluated in 45 consecutive patients with three-vessel disease with or without left main disease who underwent a CCTA 30 days (± 7 days) after CABG. The CCTA-CABG aSS was evaluated in 45 consecutive patients with 117 bypass grafts and 152 anastomoses. The median native coronary aSS was 35.0 [interquartile range (IQR) 27.0-41.0], whilst the median CCTA-CABG aSS was 13.0 (IQR 9.0-20.5). The inter-observer level of agreement for the native coronary aSS and the CCTA-CABG aSS were both substantial with respective Kappas of 0.67 and 0.61. The CCTA-CABG aSS was feasible in all patients who underwent CABG for complex coronary artery disease with substantial inter-observer reproducibility, and therefore can be used to quantify the completeness of revascularization after CABG.
Keywords: Completeness of revascularization; Coronary artery bypass graft; Coronary artery disease; Coronary computed tomographic angiography; SYNTAX Score.
© 2023. The Author(s).
Conflict of interest statement
Dr Kotoku has received a grant for studying overseas from Fukuda Foundation for Medical Technology. Dr Serruys has received consultancy fees from Philips/Volcano, SMT, Novartis, Xeltis, Merillife. Dr Masuda received a grant from Terumo Corporation outside the submitted work. Dr Narula is on the Scientific Advisory Board of HeartFlow Inc.
Figures





References
-
- Farooq V, Girasis C, Magro M, et al. The CABG SYNTAX score-an angiographic tool to grade the complexity of coronary disease following coronary artery bypass graft surgery: from the SYNTAx left main angiographic (SYNTAX-LE MANS) substudy. EuroIntervention. 2013;8:1277–1285. doi: 10.4244/EIJV8I11A196. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
