

Dual-layer dual-energy CT-derived pulmonary perfusion for the differentiation of acute pulmonary embolism and chronic thromboembolic pulmonary hypertension
- PMID: 37921925
- PMCID: PMC11126515
- DOI: 10.1007/s00330-023-10337-4
Dual-layer dual-energy CT-derived pulmonary perfusion for the differentiation of acute pulmonary embolism and chronic thromboembolic pulmonary hypertension
Abstract
Objectives: To evaluate dual-layer dual-energy computed tomography (dlDECT)-derived pulmonary perfusion maps for differentiation between acute pulmonary embolism (PE) and chronic thromboembolic pulmonary hypertension (CTEPH).
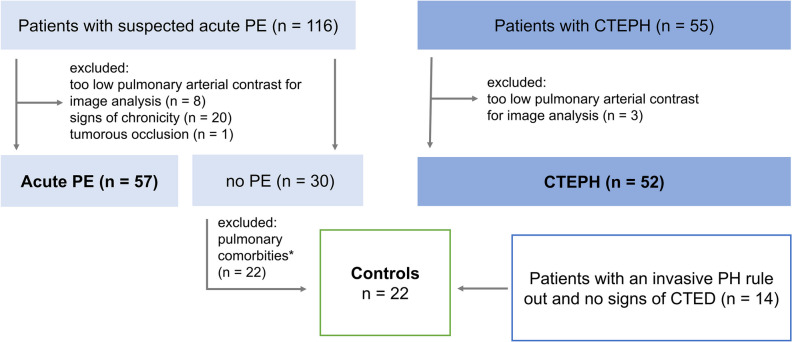
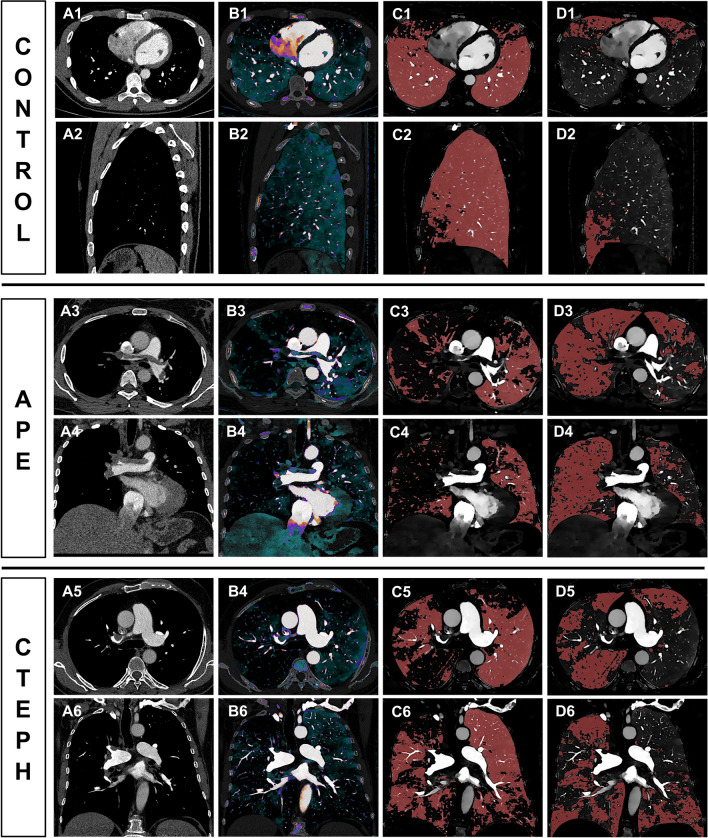
Methods: This retrospective study included 131 patients (57 patients with acute PE, 52 CTEPH, 22 controls), who underwent CT pulmonary angiography on a dlDECT. Normal and malperfused areas of lung parenchyma were semiautomatically contoured using iodine density overlay (IDO) maps. First-order histogram features of normal and malperfused lung tissue were extracted. Iodine density (ID) was normalized to the mean pulmonary artery (MPA) and the left atrium (LA). Furthermore, morphological imaging features for both acute and chronic PE, as well as the combination of histogram and morphological imaging features, were evaluated.
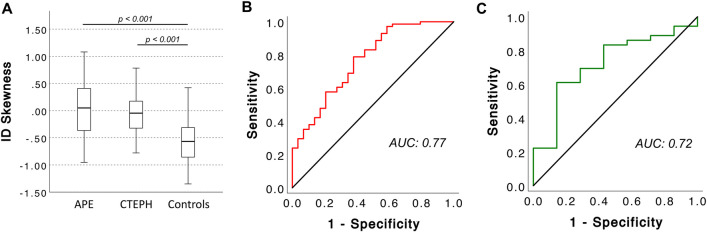
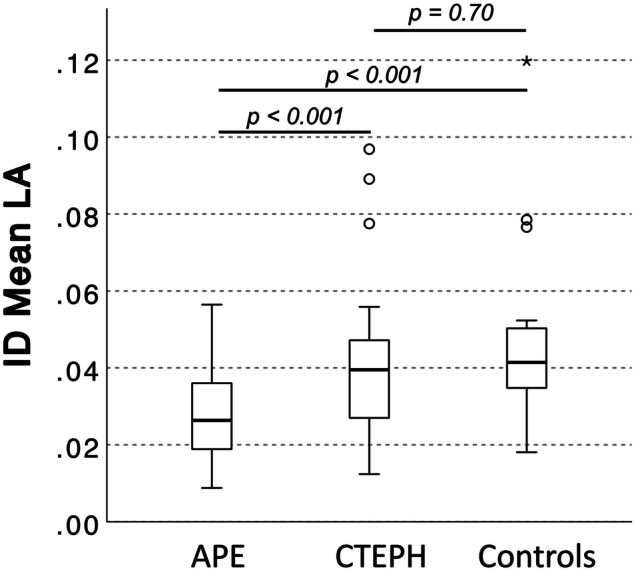
Results: In acute PE, normal perfused lung areas showed a higher mean and peak iodine uptake normalized to the MPA than in CTEPH (both p < 0.001). After normalizing mean ID in perfusion defects to the LA, patients with acute PE had a reduced average perfusion (IDmean,LA) compared to both CTEPH patients and controls (p < 0.001 for both). IDmean,LA allowed for a differentiation between acute PE and CTEPH with moderate accuracy (AUC: 0.72, sensitivity 74%, specificity 64%), resulting in a PPV and NPV for CTEPH of 64% and 70%. Combining IDmean,LA in the malperfused areas with the diameter of the MPA (MPAdia) significantly increased its ability to differentiate between acute PE and CTEPH (sole MPAdia: AUC: 0.76, 95%-CI: 0.68-0.85 vs. MPAdia + 256.3 * IDmean,LA - 40.0: AUC: 0.82, 95%-CI: 0.74-0.90, p = 0.04).
Conclusion: dlDECT enables quantification and characterization of pulmonary perfusion patterns in acute PE and CTEPH. Although these lack precision when used as a standalone criterion, when combined with morphological CT parameters, they hold potential to enhance differentiation between the two diseases.
Clinical relevance statement: Differentiating between acute PE and CTEPH based on morphological CT parameters is challenging, often leading to a delay in CTEPH diagnosis. By revealing distinct pulmonary perfusion patterns in both entities, dlDECT may facilitate timely diagnosis of CTEPH, ultimately improving clinical management.
Key points: • Morphological imaging parameters derived from CT pulmonary angiography to distinguish between acute pulmonary embolism and chronic thromboembolic pulmonary hypertension lack diagnostic accuracy. • Dual-layer dual-energy CT reveals different pulmonary perfusion patterns between acute pulmonary embolism and chronic thromboembolic pulmonary hypertension. • The identified parameters yield potential to enable more timely identification of patients with chronic thromboembolic pulmonary hypertension.
Keywords: Acute pulmonary embolism; Chronic thromboembolic pulmonary hypertension; Computed tomography; Pulmonary perfusion.
© 2023. The Author(s).
Conflict of interest statement
Simon Lennartz and Nils Große-Hokamp are members of the
Roman Johannes Gertz, Nils Große Hokamp, Lenhard Pennig, and David Maintz received speaker’s honoraria from Philips Healthcare.
Lenhard Pennig received speaker’s honoraria from Guerbet GmbH.
Figures

Similar articles
-
Dual-layer dual-energy CT characterization of thrombus composition in acute pulmonary embolism and chronic thromboembolic pulmonary hypertension.Int J Cardiovasc Imaging. 2025 Feb;41(2):303-314. doi: 10.1007/s10554-024-03309-2. Epub 2024 Dec 25. Int J Cardiovasc Imaging. 2025. PMID: 39720959 Free PMC article.
-
Morphologic and Functional Dual-Energy CT Parameters in Patients With Chronic Thromboembolic Pulmonary Hypertension and Chronic Thromboembolic Disease.AJR Am J Roentgenol. 2020 Dec;215(6):1335-1341. doi: 10.2214/AJR.19.22743. Epub 2020 Sep 29. AJR Am J Roentgenol. 2020. PMID: 32991219
-
Dual-energy CT (DECT) lung perfusion in pulmonary hypertension: concordance rate with V/Q scintigraphy in diagnosing chronic thromboembolic pulmonary hypertension (CTEPH).Eur Radiol. 2018 Dec;28(12):5100-5110. doi: 10.1007/s00330-018-5467-2. Epub 2018 May 30. Eur Radiol. 2018. PMID: 29846802
-
The diagnostic performance of dual-energy CT in detecting chronic thromboembolic pulmonary hypertension: A systematic-review and Meta-analysis.Clin Imaging. 2025 Sep;125:110552. doi: 10.1016/j.clinimag.2025.110552. Epub 2025 Jun 19. Clin Imaging. 2025. PMID: 40544642
-
Imaging of Chronic Thromboembolic Pulmonary Hypertension.Radiol Clin North Am. 2025 Mar;63(2):223-234. doi: 10.1016/j.rcl.2024.10.004. Epub 2024 Nov 12. Radiol Clin North Am. 2025. PMID: 39863376 Review.
Cited by
-
Dual-layer dual-energy CT characterization of thrombus composition in acute pulmonary embolism and chronic thromboembolic pulmonary hypertension.Int J Cardiovasc Imaging. 2025 Feb;41(2):303-314. doi: 10.1007/s10554-024-03309-2. Epub 2024 Dec 25. Int J Cardiovasc Imaging. 2025. PMID: 39720959 Free PMC article.
-
Quantitative pulmonary perfusion in acute pulmonary embolism and chronic thromboembolic pulmonary hypertension.Pulm Circ. 2024 Nov 8;14(4):e12445. doi: 10.1002/pul2.12445. eCollection 2024 Oct. Pulm Circ. 2024. PMID: 39525949 Free PMC article.
-
Development of a lung perfusion automated quantitative model based on dual-energy CT pulmonary angiography in patients with chronic pulmonary thromboembolism.Insights Imaging. 2025 Aug 18;16(1):182. doi: 10.1186/s13244-025-02067-6. Insights Imaging. 2025. PMID: 40825922 Free PMC article.
-
Fully automated Bayesian analysis for quantifying the extent and distribution of pulmonary perfusion changes on CT pulmonary angiography in CTEPH.Eur Radiol. 2025 May 28. doi: 10.1007/s00330-025-11678-y. Online ahead of print. Eur Radiol. 2025. PMID: 40437198
-
The role of ventilation/perfusion scintigraphy in distinguishing acute from chronic pulmonary embolism.Emerg Radiol. 2025 Aug 7. doi: 10.1007/s10140-025-02377-8. Online ahead of print. Emerg Radiol. 2025. PMID: 40770524
References
-
- Coquoz N, Weilenmann D, Stolz D, et al (2018) Multicentre observational screening survey for the detection of CTEPH following pulmonary embolism. Eur Respir J 51:. 10.1183/13993003.02505-2017 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
