

Deep learning system for automated detection of posterior ligamentous complex injury in patients with thoracolumbar fracture on MRI
- PMID: 37923853
- PMCID: PMC10624679
- DOI: 10.1038/s41598-023-46208-7
Deep learning system for automated detection of posterior ligamentous complex injury in patients with thoracolumbar fracture on MRI
Abstract
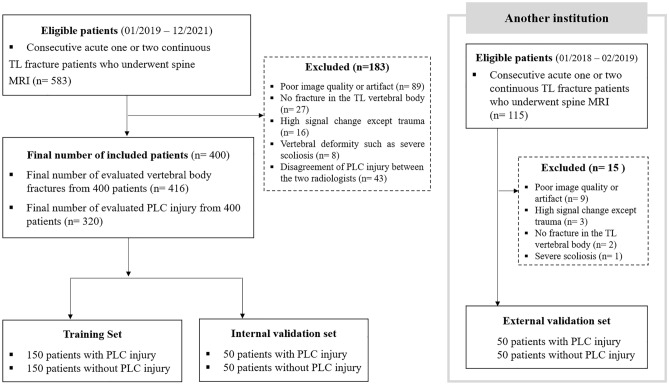
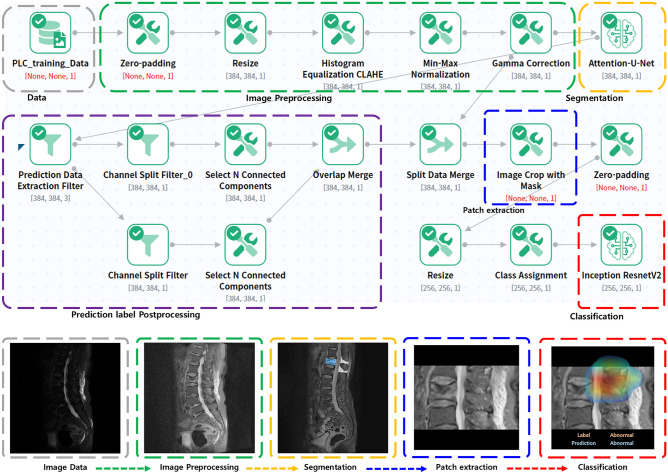
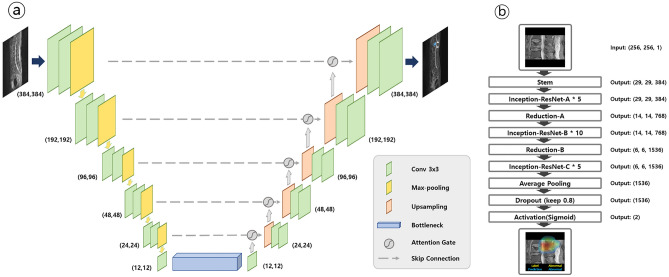
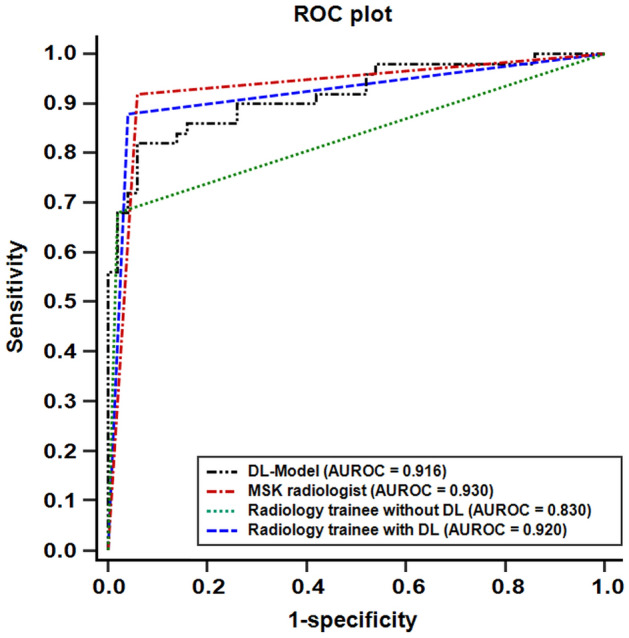
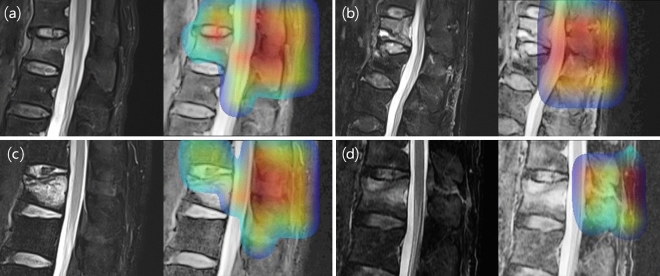
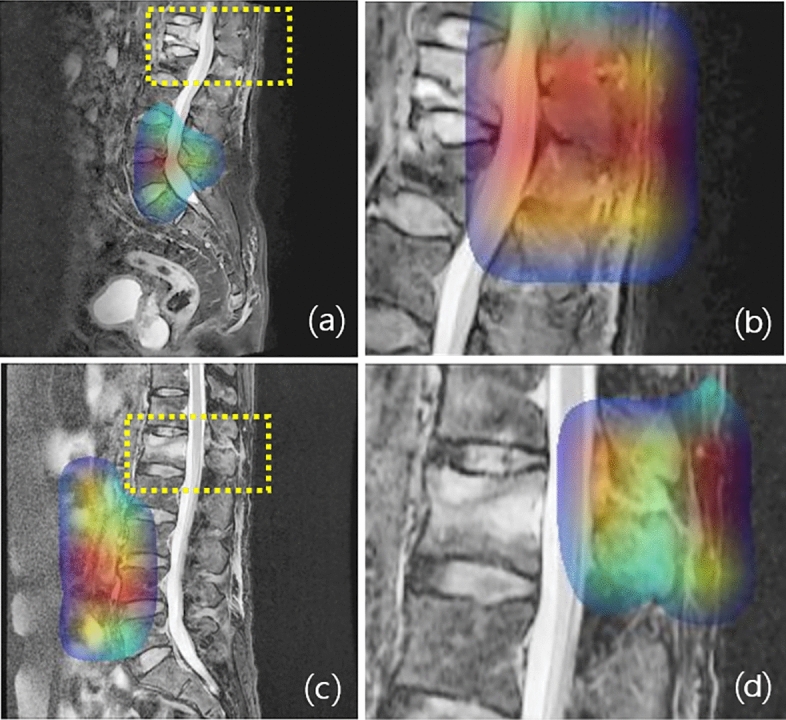
This study aimed to develop a deep learning (DL) algorithm for automated detection and localization of posterior ligamentous complex (PLC) injury in patients with acute thoracolumbar (TL) fracture on magnetic resonance imaging (MRI) and evaluate its diagnostic performance. In this retrospective multicenter study, using midline sagittal T2-weighted image with fracture (± PLC injury), a training dataset and internal and external validation sets of 300, 100, and 100 patients, were constructed with equal numbers of injured and normal PLCs. The DL algorithm was developed through two steps (Attention U-net and Inception-ResNet-V2). We evaluate the diagnostic performance for PLC injury between the DL algorithm and radiologists with different levels of experience. The area under the curves (AUCs) generated by the DL algorithm were 0.928, 0.916 for internal and external validations, and by two radiologists for observer performance test were 0.930, 0.830, respectively. Although no significant difference was found in diagnosing PLC injury between the DL algorithm and radiologists, the DL algorithm exhibited a trend of higher AUC than the radiology trainee. Notably, the radiology trainee's diagnostic performance significantly improved with DL algorithm assistance. Therefore, the DL algorithm exhibited high diagnostic performance in detecting PLC injuries in acute TL fractures.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Diagnostic accuracy of magnetic resonance imaging for detecting posterior ligamentous complex injury associated with thoracic and lumbar fractures.J Neurosurg. 2003 Jul;99(1 Suppl):20-6. doi: 10.3171/spi.2003.99.1.0020. J Neurosurg. 2003. PMID: 12859054
-
Which Morphological Features of Facet Diastasis Predict Thoracolumbar Posterior Ligamentous Complex Injury as Defined by Magnetic Resonance Imaging?World Neurosurg. 2023 Mar;171:e276-e285. doi: 10.1016/j.wneu.2022.12.010. Epub 2022 Dec 13. World Neurosurg. 2023. PMID: 36521759
-
Relationships between posterior ligamentous complex injury and radiographic parameters in patients with thoracolumbar burst fractures.Injury. 2015 Feb;46(2):392-8. doi: 10.1016/j.injury.2014.10.047. Epub 2014 Oct 22. Injury. 2015. PMID: 25457338
-
Prediction of MRI findings including disc injury and posterior ligamentous complex injury in neurologically intact thoracolumbar burst fractures by the parameters of vertebral body damage on CT scan.Injury. 2018 Feb;49(2):272-278. doi: 10.1016/j.injury.2017.12.011. Epub 2017 Dec 15. Injury. 2018. PMID: 29290375
-
Towards a standardized reporting of the impact of magnetic resonance imaging on the decision-making of thoracolumbar fractures without neurological deficit: Conceptual framework and proposed methodology.Brain Spine. 2024 Mar 21;4:102787. doi: 10.1016/j.bas.2024.102787. eCollection 2024. Brain Spine. 2024. PMID: 38590587 Free PMC article. Review.
Cited by
-
Applications of Artificial Intelligence and Machine Learning in Spine MRI.Bioengineering (Basel). 2024 Sep 5;11(9):894. doi: 10.3390/bioengineering11090894. Bioengineering (Basel). 2024. PMID: 39329636 Free PMC article. Review.
-
Sensitivity and specificity of machine learning and deep learning algorithms in the diagnosis of thoracolumbar injuries resulting in vertebral fractures: A systematic review and meta-analysis.Brain Spine. 2024 Apr 17;4:102809. doi: 10.1016/j.bas.2024.102809. eCollection 2024. Brain Spine. 2024. PMID: 38681175 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
