

Guidelines for Neuroprognostication in Critically Ill Adults with Intracerebral Hemorrhage
- PMID: 37923968
- PMCID: PMC10959839
- DOI: 10.1007/s12028-023-01854-7
Guidelines for Neuroprognostication in Critically Ill Adults with Intracerebral Hemorrhage
Abstract
Background: The objective of this document is to provide recommendations on the formal reliability of major clinical predictors often associated with intracerebral hemorrhage (ICH) neuroprognostication.
Methods: A narrative systematic review was completed using the Grading of Recommendations Assessment, Development, and Evaluation methodology and the Population, Intervention, Comparator, Outcome, Timing, Setting questions. Predictors, which included both individual clinical variables and prediction models, were selected based on clinical relevance and attention in the literature. Following construction of the evidence profile and summary of findings, recommendations were based on Grading of Recommendations Assessment, Development, and Evaluation criteria. Good practice statements addressed essential principles of neuroprognostication that could not be framed in the Population, Intervention, Comparator, Outcome, Timing, Setting format.
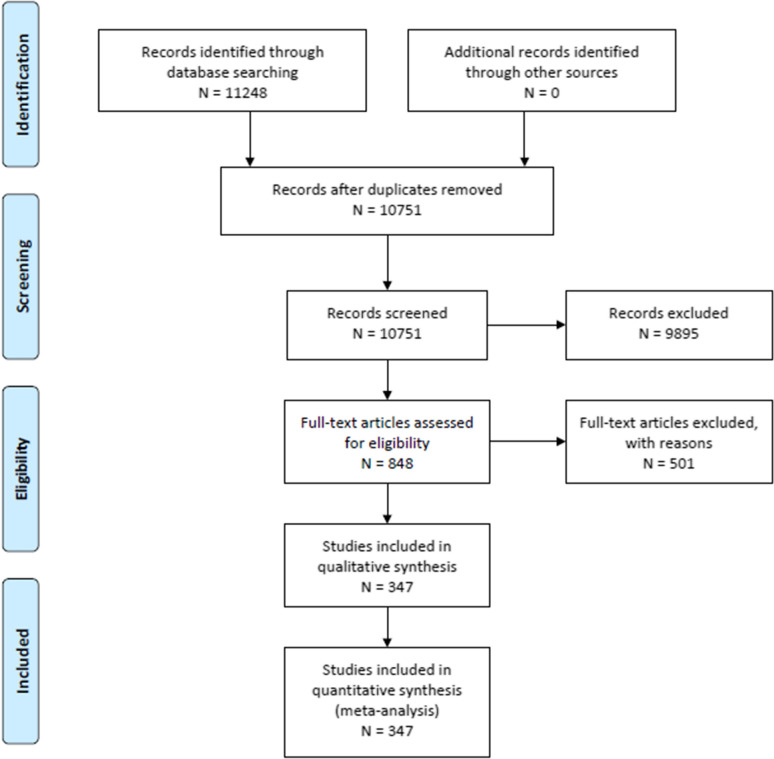
Results: Six candidate clinical variables and two clinical grading scales (the original ICH score and maximally treated ICH score) were selected for recommendation creation. A total of 347 articles out of 10,751 articles screened met our eligibility criteria. Consensus statements of good practice included deferring neuroprognostication-aside from the most clinically devastated patients-for at least the first 48-72 h of intensive care unit admission; understanding what outcomes would have been most valued by the patient; and counseling of patients and surrogates whose ultimate neurological recovery may occur over a variable period of time. Although many clinical variables and grading scales are associated with ICH poor outcome, no clinical variable alone or sole clinical grading scale was suggested by the panel as currently being reliable by itself for use in counseling patients with ICH and their surrogates, regarding functional outcome at 3 months and beyond or 30-day mortality.
Conclusions: These guidelines provide recommendations on the formal reliability of predictors of poor outcome in the context of counseling patients with ICH and surrogates and suggest broad principles of neuroprognostication. Clinicians formulating their judgments of prognosis for patients with ICH should avoid anchoring bias based solely on any one clinical variable or published clinical grading scale.
Keywords: Cerebral hemorrhage; Counseling; Critical care outcomes; Hemorrhagic stroke; Mortality; Patient outcome assessment; Practice guideline; Prognosis; Shared decision making.
© 2023. The Author(s).
Conflict of interest statement
GVF reports clinical consultant fees and speaker honoraria from AstraZeneca and clinical consultant fees from Chiesi. DYH reports pilot research grant funding from the Neurocritical Care Foundation. No other authors have any conflicts to disclose related to the content of this manuscript. These guidelines were endorsed by the Society of Critical Care Medicine and the Deutsche Gesellschaft für Neurochirurgie (German Society of Neurosurgery).
Figures
References
-
- van Asch CJ, Luitse MJ, Rinkel GJ, et al. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9(2):167–176. - PubMed
-
- Bako AT, Pan A, Potter T, et al. Contemporary trends in the nationwide incidence of primary intracerebral hemorrhage. Stroke. 2022;53(3):e70–e74. - PubMed
-
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2022 update: a report From the American Heart Association. Circulation. 2022;145(8):e153–e639. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
