

Management of asymptomatic sexually transmitted infections in Europe: towards a differentiated, evidence-based approach
- PMID: 37927435
- PMCID: PMC10624996
- DOI: 10.1016/j.lanepe.2023.100743
Management of asymptomatic sexually transmitted infections in Europe: towards a differentiated, evidence-based approach
Abstract
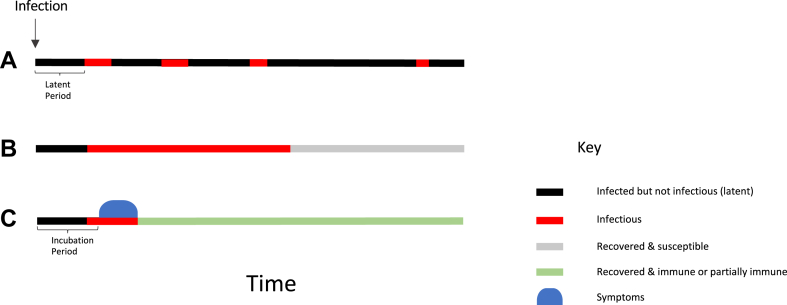
Most sexually transmitted infections (STIs) can be accurately diagnosed and treated during asymptomatic carriage. Widespread screening for these STIs is therefore assumed to be an effective way to reduce their prevalence and associated disease. In this review, we provide evidence that this is the case for HIV and syphilis. However, for other STIs such as Neisseria gonorrhoeae and Chlamydia trachomatis, our review reveals that the evidence that screening reduces infection prevalence and associated disease is weak. There is also growing evidence of harms from screening that might outweigh any benefits. The harms include the increased consumption of antimicrobials that follows frequent screening and increased detection of asymptomatic STIs in key populations, such as men who have sex with men taking HIV pre-exposure prophylaxis, and associated risk of antimicrobial resistance in target and non-target organisms. There may also be psycho-social harm associated with an STI diagnosis. We conclude that in the absence of symptoms, in high STI prevalence populations frequent STI screening should be limited to HIV and syphilis.
© 2023 The Author(s).
Conflict of interest statement
All authors declare that they have no conflicts of interest. GH is the PI at London School of Hygiene and Tropical Medicine (LSHTM) on funding for the UK Public Health Rapid Support Team, which is funded by Official Development Assistance (ODA) via the Department of Health and Social Care & the National Institute for Health Research (NIHR) Central Commissions Facility.
Figures
References
-
- Korenromp E.L., Sudaryo M.K., de Vlas S.J., et al. What proportion of episodes of gonorrhoea and chlamydia becomes symptomatic? Int J STD AIDS. 2002;13(2):91–101. - PubMed
-
- Zeggagh J., Bauer R., Delaugerre C., et al. Incidence and risk factors for recurrent sexually transmitted infections among MSM on HIV pre-exposure prophylaxis. AIDS. 2022;36(8):1129–1134. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
