

Comparative effectiveness of nirmatrelvir/ritonavir versus sotrovimab and molnupiravir for preventing severe COVID-19 outcomes in non-hospitalised high-risk patients during Omicron waves: observational cohort study using the OpenSAFELY platform
- PMID: 37927438
- PMCID: PMC10624988
- DOI: 10.1016/j.lanepe.2023.100741
Comparative effectiveness of nirmatrelvir/ritonavir versus sotrovimab and molnupiravir for preventing severe COVID-19 outcomes in non-hospitalised high-risk patients during Omicron waves: observational cohort study using the OpenSAFELY platform
Abstract
Background: Timely evidence of the comparative effectiveness between COVID-19 therapies in real-world settings is needed to inform clinical care. This study aimed to compare the effectiveness of nirmatrelvir/ritonavir versus sotrovimab and molnupiravir in preventing severe COVID-19 outcomes in non-hospitalised high-risk COVID-19 adult patients during Omicron waves.
Methods: With the approval of NHS England, we conducted a real-world cohort study using the OpenSAFELY-TPP platform. Patient-level primary care data were obtained from 24 million people in England and were securely linked with data on COVID-19 infection and therapeutics, hospital admission, and death, covering a period where both nirmatrelvir/ritonavir and sotrovimab were first-line treatment options in community settings (February 10, 2022-November 27, 2022). Molnupiravir (third-line option) was used as an exploratory comparator to nirmatrelvir/ritonavir, both of which were antivirals. Cox proportional hazards model stratified by area was used to compare the risk of 28-day COVID-19 related hospitalisation/death across treatment groups.
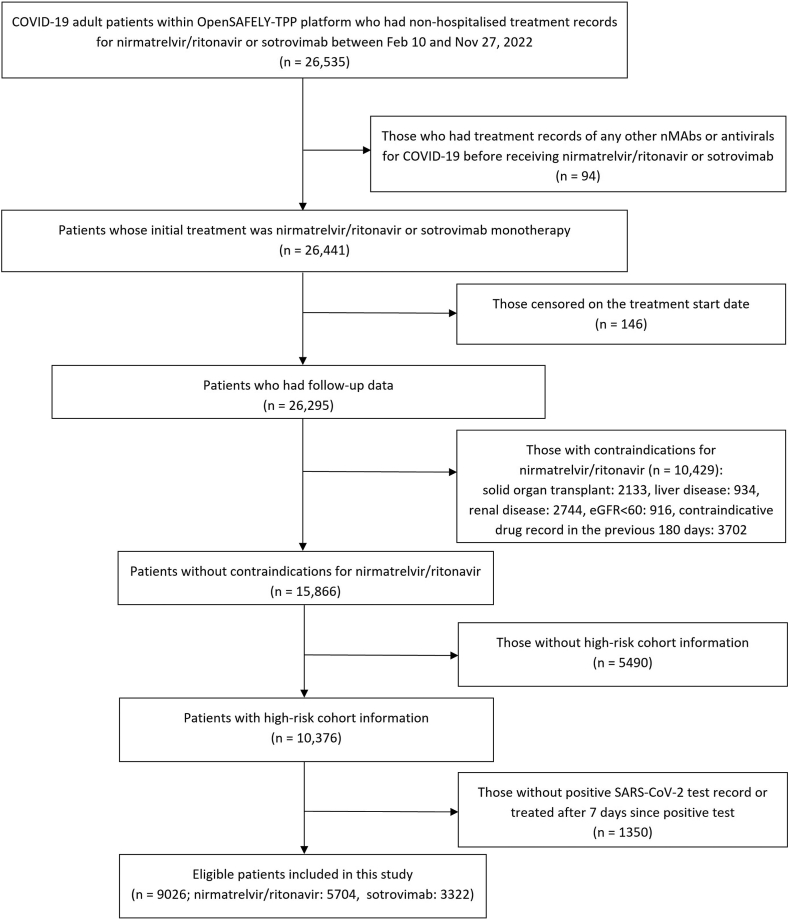
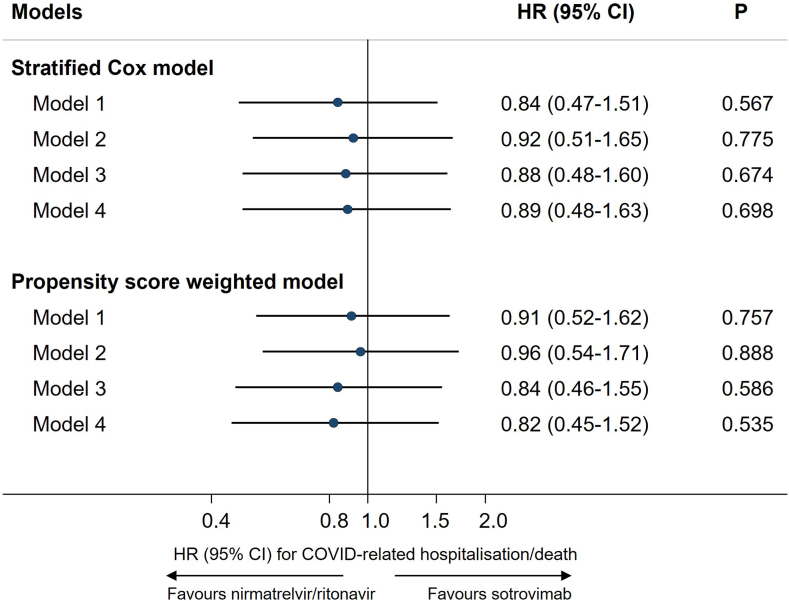
Findings: A total of 9026 eligible patients treated with nirmatrelvir/ritonavir (n = 5704) and sotrovimab (n = 3322) were included in the main analysis. The mean age was 52.7 (SD = 14.9) years and 93% (8436/9026) had three or more COVID-19 vaccinations. Within 28 days after treatment initiation, 55/9026 (0.61%) COVID-19 related hospitalisations/deaths were observed (34/5704 [0.60%] treated with nirmatrelvir/ritonavir and 21/3322 [0.63%] with sotrovimab). After adjusting for demographics, high-risk cohort categories, vaccination status, calendar time, body mass index and other comorbidities, we observed no significant difference in outcome risk between nirmatrelvir/ritonavir and sotrovimab users (HR = 0.89, 95% CI: 0.48-1.63; P = 0.698). Results from propensity score weighted model also showed non-significant difference between treatment groups (HR = 0.82, 95% CI: 0.45-1.52; P = 0.535). The exploratory analysis comparing nirmatrelvir/ritonavir users with 1041 molnupiravir users (13/1041 [1.25%] COVID-19 related hospitalisations/deaths) showed an association in favour of nirmatrelvir/ritonavir (HR = 0.45, 95% CI: 0.22-0.94; P = 0.033).
Interpretation: In routine care of non-hospitalised high-risk adult patients with COVID-19 in England, no substantial difference in the risk of severe COVID-19 outcomes was observed between those who received nirmatrelvir/ritonavir and sotrovimab between February and November 2022, when Omicron subvariants BA.2, BA.5, or BQ.1 were dominant.
Funding: UK Research and Innovation, Wellcome Trust, UK Medical Research Council, National Institute for Health and Care Research, and Health Data Research UK.
Keywords: COVID-19; Comparative effectiveness; Paxlovid; Real-world data; Sotrovimab.
© 2023 The Author(s).
Conflict of interest statement
BG has received research funding from the Laura and John Arnold Foundation, the NHS National Institute for Health Research (NIHR), the NIHR School of Primary Care Research, NHS England, the NIHR Oxford Biomedical Research Centre, the Mohn-Westlake Foundation, NIHR Applied Research Collaboration Oxford and Thames Valley, the Wellcome Trust, the Good Thinking Foundation, Health Data Research UK, the Health Foundation, the World Health Organisation, UKRI MRC, Asthma UK, the British Lung Foundation, and the Longitudinal Health and Wellbeing strand of the National Core Studies programme; he is a Non-Executive Director at NHS Digital; he also receives personal income from speaking and writing for lay audiences on the misuse of science. BMK is also employed by NHS England working on medicines policy and clinical lead for primary care medicines data. AM is a member of RCGP health informatics group and the NHS Digital GP data Professional Advisory Group, and received consulting fee from Induction Healthcare. SJWE was paid for attendance at meetings of Coalition for Epidemic Preparedness Innovations (CEPI) Meta–Data Safety Monitoring Board. IJD has received research grants from GSK and AstraZeneca and holds shares in GSK. LAT has received research funding from MRC, Wellcome, NIHR and GSK, consulted for Bayer in relation to an observational study of chronic kidney disease (unpaid), and is a member of 4 non-industry funded (NIHR/MRC) trial advisory committees (unpaid) and MHRA Expert advisory group (Women’s Health). ELH received NIHR post doctoral fellowship. REC has shares in AstraZeneca. VM received grant from NIHR. VS received speaker fees from Bayer AG. JP is employed by TPP SystmOne in the role of Clinical Director. RME received research grants from NIHR, HDR UK, IMI2, New Ventures Fund. JT received AstraZeneca grant for unrelated COVID-19 research. Other authors declared no conflict of interest.
Figures
References
-
- NHS Neutralising monoclonal antibodies (nMABs) or antivirals for non-hospitalised patients with COVID-19. 2021. https://www.cas.mhra.gov.uk/ViewandAcknowledgment/ViewAlert.aspx?AlertID...
-
- NHS Antivirals or neutralising antibodies for non-hospitalised patients with COVID-19. 2022. https://www.cas.mhra.gov.uk/ViewandAcknowledgment/ViewAlert.aspx?AlertID...
Grants and funding
LinkOut - more resources
Full Text Sources
