

Advancing pharmacogenetic testing in a tertiary hospital: a retrospective analysis after 10 years of activity
- PMID: 37927587
- PMCID: PMC10622662
- DOI: 10.3389/fphar.2023.1292416
Advancing pharmacogenetic testing in a tertiary hospital: a retrospective analysis after 10 years of activity
Abstract
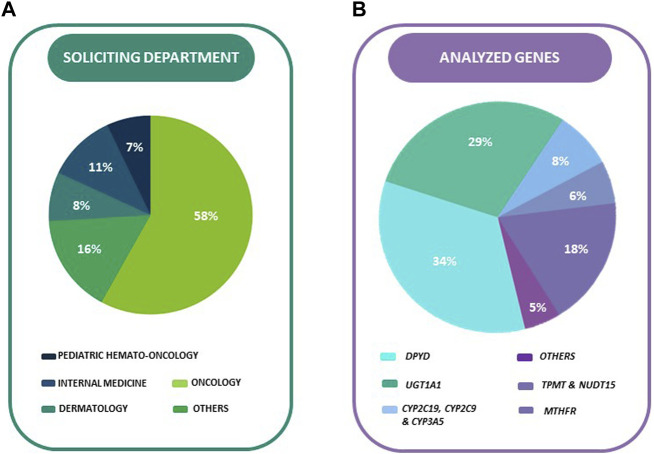
The field of pharmacogenetics (PGx) holds great promise in advancing personalized medicine by adapting treatments based on individual genetic profiles. Despite its benefits, there are still economic, ethical and institutional barriers that hinder its implementation in our healthcare environment. A retrospective analysis approach of anonymized data sourced from electronic health records was performed, encompassing a diverse patient population and evaluating key parameters such as prescribing patterns and test results, to assess the impact of pharmacogenetic testing. A head-to-head comparison with previously published activity results within the same pharmacogenetic laboratory was also conducted to contrast the progress made after 10 years. The analysis revealed significant utilization of pharmacogenetic testing in daily clinical practice, with 1,145 pharmacogenetic tests performed over a 1-year period and showing a 35% growth rate increase over time. Of the 17 different medical departments that sought PGx tests, the Oncology department accounted for the highest number, representing 58.47% of all genotyped patients. A total of 1,000 PGx tests were requested for individuals susceptible to receive a dose modification based on genotype, and 76 individuals received a genotype-guided dose adjustment. This study presents a comprehensive descriptive analysis of real-world data obtained from a public tertiary hospital laboratory specialized in pharmacogenetic testing, and presents data that strongly endorse the integration of pharmacogenetic testing into everyday clinical practice.
Keywords: personalized medicine; pharmacogenetic dosing; preemptive genotyping; real-world data; retrospective analysis.
Copyright © 2023 Stewart, Dodero-Anillo, Guijarro-Eguinoa, Arias, Gómez López De Las Huertas, Seco-Meseguer, García-García, Ramírez García, Rodríguez-Antolín, Carcas, Rodriguez-Novoa, Rosas-Alonso and Borobia.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Agencia Española del Medicamento y Productos Sanitarios (AEMPS) (2020). Security Alert: fluorouracil, capecitabine, tegafur, and flucytosine in patients with dihydropyrimidine dehydrogenase deficiency. Available at: https://www.aemps.gob.es/informa-en/fluorouracilo-capecitabina-tegafur-y... (Accessed June 16, 2023).
-
- Bielinski S. J., Olson J. E., Pathak J., Weinshilboum R. M., Wang L., Lyke K. J., et al. (2014). Preemptive genotyping for personalized medicine: design of the right drug, right dose, right time-using genomic data to individualize treatment protocol. Mayo Clin. Proc. 89, 25–33. 10.1016/J.MAYOCP.2013.10.021 - DOI - PMC - PubMed
-
- Bignucolo A., De Mattia E., Roncato R., Peruzzi E., Scarabel L., D’Andrea M., et al. (2023). Ten-year experience with pharmacogenetic testing for DPYD in a national cancer center in Italy: lessons learned on the path to implementation. Front. Pharmacol. 14, 1199462. 10.3389/fphar.2023.1199462 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources