

Differential drug response in pulmonary arterial hypertension: The potential for precision medicine
- PMID: 37927610
- PMCID: PMC10621006
- DOI: 10.1002/pul2.12304
Differential drug response in pulmonary arterial hypertension: The potential for precision medicine
Abstract
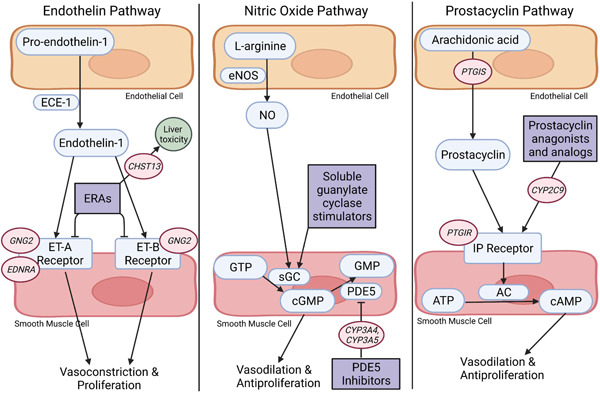
Pulmonary arterial hypertension (PAH) is a rare, complex, and deadly cardiopulmonary disease. It is characterized by changes in endothelial cell function and smooth muscle cell proliferation in the pulmonary arteries, causing persistent vasoconstriction, resulting in right heart hypertrophy and failure. There are multiple drug classes specific to PAH treatment, but variation between patients may impact treatment response. A small subset of patients is responsive to pulmonary vasodilators and can be treated with calcium channel blockers, which would be deleterious if prescribed to a typical PAH patient. Little is known about the underlying cause of this important difference in vasoresponsive PAH patients. Sex, race/ethnicity, and pharmacogenomics may also factor into efficacy and safety of PAH-specific drugs. Research has indicated that endothelin receptor antagonists may be more effective in women and there have been some minor differences found in certain races and ethnicities, but these findings are muddled by the impact of socioeconomic factors and a lack of representation of non-White patients in clinical trials. Genetic variants in genes such as CYP3A5, CYP2C9, PTGIS, PTGIR, GNG2, CHST3, and CHST13 may influence the efficacy and safety of certain PAH-specific drugs. PAH research faces many challenges, but there is potential for new methodologies to glean new insights into PAH development and treatment.
Keywords: diverse populations; pharmacogenomics; pharmacotherapy; pulmonary arterial hypertension.
© 2023 The Authors. Pulmonary Circulation published by John Wiley & Sons Ltd on behalf of Pulmonary Vascular Research Institute.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Benza RL, Miller DP, Barst RJ, Badesch DB, Frost AE, McGoon MD. An evaluation of long‐term survival from time of diagnosis in pulmonary arterial hypertension from the REVEAL registry. Chest. 2012;142(2):448–456. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
