

Evaluating the impact of testing strategies for the detection of nosocomial COVID-19 in English hospitals through data-driven modeling
- PMID: 37928455
- PMCID: PMC10622791
- DOI: 10.3389/fmed.2023.1166074
Evaluating the impact of testing strategies for the detection of nosocomial COVID-19 in English hospitals through data-driven modeling
Abstract
Introduction: During the first wave of the COVID-19 pandemic 293,204 inpatients in England tested positive for SARS-CoV-2. It is estimated that 1% of these cases were hospital-associated using European centre for disease prevention and control (ECDC) and Public Health England (PHE) definitions. Guidelines for preventing the spread of SARS-CoV-2 in hospitals have developed over time but the effectiveness and efficiency of testing strategies for preventing nosocomial transmission has not been explored.
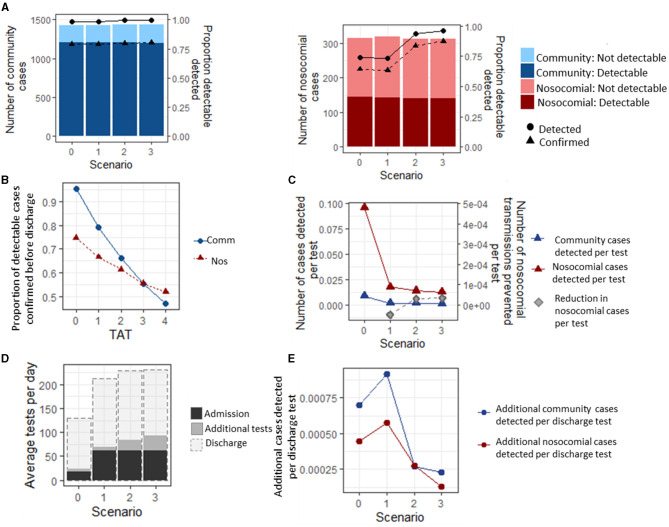
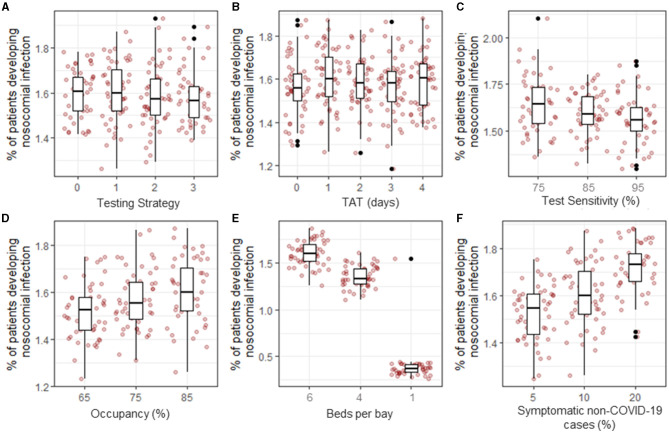
Methods: Using an individual-based model, parameterised using multiple datasets, we simulated the transmission of SARS-CoV-2 to patients and healthcare workers between March and August 2020 and evaluated the efficacy of different testing strategies. These strategies were: 0) Testing only symptomatic patients on admission; 1) Testing all patients on admission; 2) Testing all patients on admission and again between days 5 and 7, and 3) Testing all patients on admission, and again at days 3, and 5-7. In addition to admissions testing, patients that develop a symptomatic infection while in hospital were tested under all strategies. We evaluated the impact of testing strategy, test characteristics and hospital-related factors on the number of nosocomial patient infections.
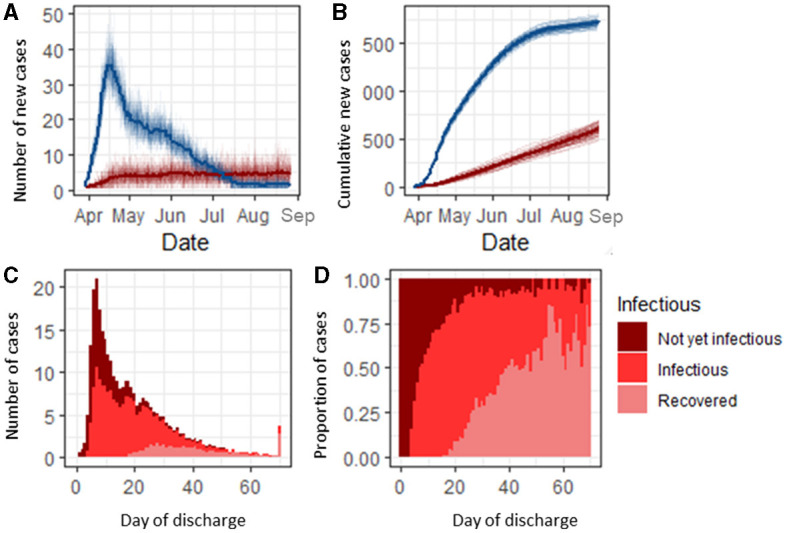
Results: Modelling suggests that 84.6% (95% CI: 84.3, 84.7) of community-acquired and 40.8% (40.3, 41.3) of hospital-associated SARS-CoV-2 infections are detectable before a patient is discharged from hospital. Testing all patients on admission and retesting after 3 or 5 days increases the proportion of nosocomial cases detected by 9.2%. Adding discharge testing increases detection by a further 1.5% (relative increase). Increasing occupancy rates, number of beds per bay, or the proportion of admissions wrongly suspected of having COVID-19 on admission and therefore incorrectly cohorted with COVID-19 patients, increases the rate of nosocomial transmission. Over 30,000 patients in England could have been discharged while incubating a non-detected SARS-CoV-2 infection during the first wave of the COVID-19 pandemic, of which 3.3% could have been identified by discharge screening. There was no significant difference in the rates of nosocomial transmission between testing strategies or when the turnaround time of the test was increased.
Discussion: This study provides insight into the efficacy of testing strategies in a period unbiased by vaccines and variants. The findings are relevant as testing programs for SARS-CoV-2 are scaled back, and possibly if a new vaccine escaping variant emerges.
Keywords: COVID-19; SARS-CoV-2; hospital-associated (or hospital-acquired) infection; modeling; nosocomial transmission; testing.
Copyright © 2023 Evans, Stimson, Pople, Wilcox, Hope and Robotham.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The effectiveness and efficiency of asymptomatic SARS-CoV-2 testing strategies for patient and healthcare workers within acute NHS hospitals during an omicron-like period.BMC Infect Dis. 2024 Jan 8;24(1):64. doi: 10.1186/s12879-023-08948-9. BMC Infect Dis. 2024. PMID: 38191324 Free PMC article.
-
Impact of interventions to reduce nosocomial transmission of SARS-CoV-2 in English NHS Trusts: a computational modelling study.BMC Infect Dis. 2024 May 7;24(1):475. doi: 10.1186/s12879-024-09330-z. BMC Infect Dis. 2024. PMID: 38714946 Free PMC article.
-
Assessment of Hospital-Onset SARS-CoV-2 Infection Rates and Testing Practices in the US, 2020-2022.JAMA Netw Open. 2023 Aug 1;6(8):e2329441. doi: 10.1001/jamanetworkopen.2023.29441. JAMA Netw Open. 2023. PMID: 37639273 Free PMC article.
-
The contribution of hospital-acquired infections to the COVID-19 epidemic in England in the first half of 2020.BMC Infect Dis. 2022 Jun 18;22(1):556. doi: 10.1186/s12879-022-07490-4. BMC Infect Dis. 2022. PMID: 35717168 Free PMC article.
-
A Systematic Review and Meta-Analysis of Inpatient Mortality Associated With Nosocomial and Community COVID-19 Exposes the Vulnerability of Immunosuppressed Adults.Front Immunol. 2021 Oct 6;12:744696. doi: 10.3389/fimmu.2021.744696. eCollection 2021. Front Immunol. 2021. PMID: 34691049 Free PMC article.
Cited by
-
Comparing the effectiveness of universal admission testing and risk-based testing at emergency admission for preventing nosocomial COVID-19: a multicenter retrospective cohort study in Japan.Infect Control Hosp Epidemiol. 2024 Oct 22;46(1):1-9. doi: 10.1017/ice.2024.161. Online ahead of print. Infect Control Hosp Epidemiol. 2024. PMID: 39434373 Free PMC article.
-
Evaluating pooled testing for asymptomatic screening of healthcare workers in hospitals.BMC Infect Dis. 2023 Dec 21;23(1):900. doi: 10.1186/s12879-023-08881-x. BMC Infect Dis. 2023. PMID: 38129789 Free PMC article.
-
The effectiveness and efficiency of asymptomatic SARS-CoV-2 testing strategies for patient and healthcare workers within acute NHS hospitals during an omicron-like period.BMC Infect Dis. 2024 Jan 8;24(1):64. doi: 10.1186/s12879-023-08948-9. BMC Infect Dis. 2024. PMID: 38191324 Free PMC article.
References
-
- Chaturvedi R, Chhibber-Goel J, Malhotra S, Sharma A. A perspective on SARS-CoV-2 and community transmission in the top COVID-19 affected nations. J Glob Health Rep. (2021) 5:e2021083. 10.29392/001c.27141 - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous