

Percutaneous Revascularization for Ischemic Left Ventricular Dysfunction: Cost-Effectiveness Analysis of the REVIVED-BCIS2 Trial
- PMID: 37929587
- PMCID: PMC10782932
- DOI: 10.1161/CIRCOUTCOMES.123.010533
Percutaneous Revascularization for Ischemic Left Ventricular Dysfunction: Cost-Effectiveness Analysis of the REVIVED-BCIS2 Trial
Abstract
Background: Percutaneous coronary intervention (PCI) is frequently undertaken in patients with ischemic left ventricular systolic dysfunction. The REVIVED (Revascularization for Ischemic Ventricular Dysfunction)-BCIS2 (British Cardiovascular Society-2) trial concluded that PCI did not reduce the incidence of all-cause death or heart failure hospitalization; however, patients assigned to PCI reported better initial health-related quality of life than those assigned to optimal medical therapy (OMT) alone. The aim of this study was to assess the cost-effectiveness of PCI+OMT compared with OMT alone.
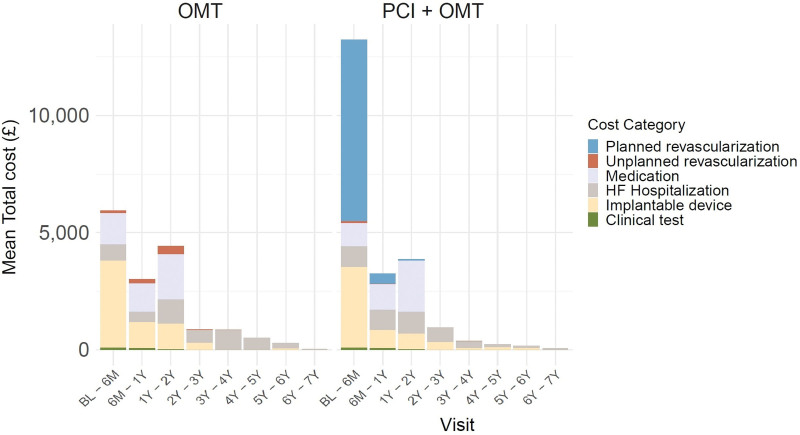
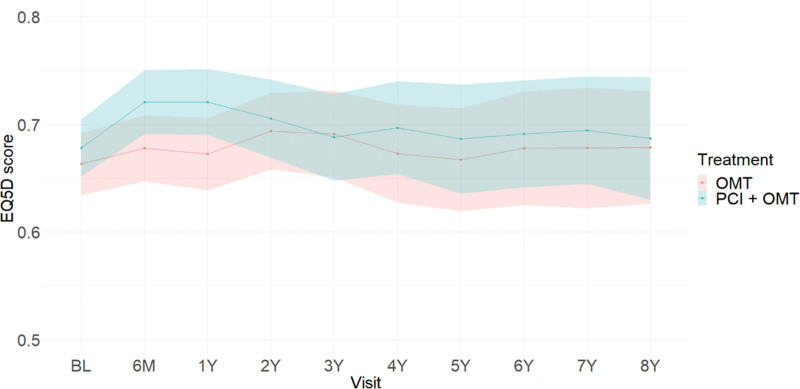
Methods: REVIVED-BCIS2 was a prospective, multicenter UK trial, which randomized patients with severe ischemic left ventricular systolic dysfunction to either PCI+OMT or OMT alone. Health care resource use (including planned and unplanned revascularizations, medication, device implantation, and heart failure hospitalizations) and health outcomes data (EuroQol 5-dimension 5-level questionnaire) on each patient were collected at baseline and up to 8 years post-randomization. Resource use was costed using publicly available national unit costs. Within the trial, mean total costs and quality-adjusted life-years (QALYs) were estimated from the perspective of the UK health system. Cost-effectiveness was evaluated using estimated mean costs and QALYs in both groups. Regression analysis was used to adjust for clinically relevant predictors.
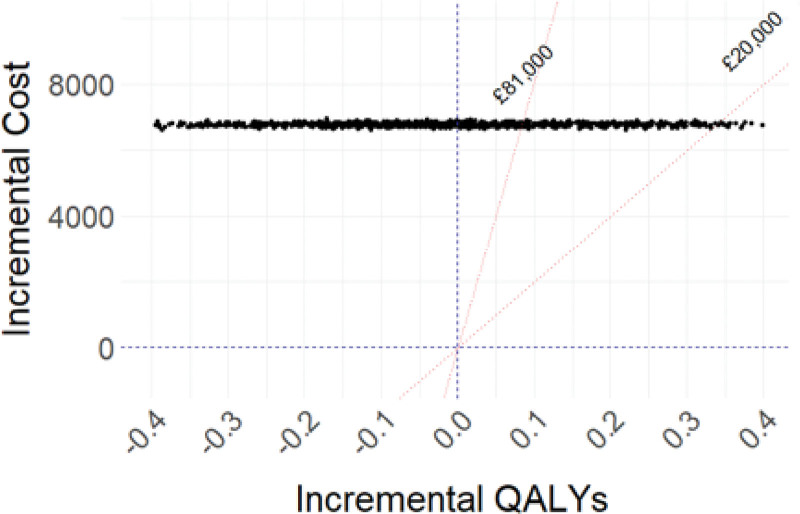
Results: Between 2013 and 2020, 700 patients were recruited (mean age: PCI+OMT=70 years, OMT=68 years; male (%): PCI+OMT=87, OMT=88); median follow-up was 3.4 years. Over all follow-ups, patients undergoing PCI yielded similar health benefits at higher costs compared with OMT alone (PCI+OMT: 4.14 QALYs, £22 352; OMT alone: 4.16 QALYs, £15 569; difference: -0.015, £6782). For both groups, most health resource consumption occurred in the first 2 years post-randomization. Probabilistic results showed that the probability of PCI being cost-effective was 0.
Conclusions: A minimal difference in total QALYs was identified between arms, and PCI+OMT was not cost-effective compared with OMT, given its additional cost. A strategy of routine PCI to treat ischemic left ventricular systolic dysfunction does not seem to be a justifiable use of health care resources in the United Kingdom.
Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT01920048.
Keywords: coronary artery disease; heart failure; humans; myocardial revascularization; percutaneous coronary intervention.
Conflict of interest statement
Figures
Comment in
-
Percutaneous Coronary Intervention for Heart Failure: Worth the Cost?Circ Cardiovasc Qual Outcomes. 2024 Jan;17(1):e010572. doi: 10.1161/CIRCOUTCOMES.123.010572. Epub 2023 Nov 6. Circ Cardiovasc Qual Outcomes. 2024. PMID: 37929590 Free PMC article. No abstract available.
References
-
- British Heart Foundation. UK factsheet. 2023:1–21. Accessed September 20, 2023. Available at https://www.bhf.org.uk/-/media/files/for-professionals/research/heart-st...
-
- Chew DS, Cowper PA, Al-Khalidi H, Anstrom KJ, Daniels MR, Davidson-Ray L, Li Y, Michler RE, Panza JA, Piña IL, et al. . Cost-effectiveness of coronary artery bypass surgery versus medicine in ischemic cardiomyopathy: the STICH randomized clinical trial. Circulation. 2022;145:819–828. doi: 10.1161/CIRCULATIONAHA.121.056276 - PMC - PubMed
-
- Perera D, Clayton T, Petrie MC, Greenwood JP, O’Kane PD, Evans R, Sculpher M, Mcdonagh T, Gershlick A, de Belder M, et al. . Percutaneous revascularization for ischemic ventricular dysfunction: rationale and design of the REVIVED-BCIS2 trial. JACC Heart Fail. 2018;6:517–526. doi: 10.1016/j.jchf.2018.01.024 - PubMed
-
- Perera D, Clayton T, O’Kane PD, Greenwood JP, Weerackody R, Ryan M, Morgan HP, Dodd M, Evans R, Canter R, et al. ; REVIVED-BCIS2 Investigators. Percutaneous revascularization for ischemic left ventricular dysfunction. N Engl J Med. 2022;387:1351–1360. doi: 10.1056/NEJMoa2206606 - PubMed
-
- Pathak S, Lai FY, Miksza J, Petrie MC, Roman M, Murray S, Dearling J, Perera D, Murphy GJ. Surgical or percutaneous coronary revascularization for heart failure: an in silico model using routinely collected health data to emulate a clinical trial. Eur Heart J. 2023;44:351–364. doi: 10.1093/eurheartj/ehac670 - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
