

Temporal Trends in Heart Failure Management and Outcomes: Insights From a Japanese Multicenter Registry of Tertiary Care Centers
- PMID: 37929712
- PMCID: PMC10727373
- DOI: 10.1161/JAHA.123.031179
Temporal Trends in Heart Failure Management and Outcomes: Insights From a Japanese Multicenter Registry of Tertiary Care Centers
Abstract
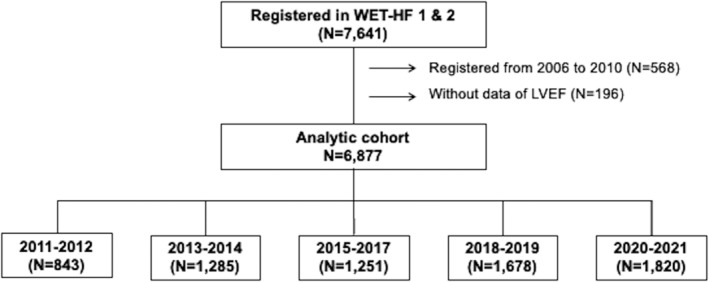
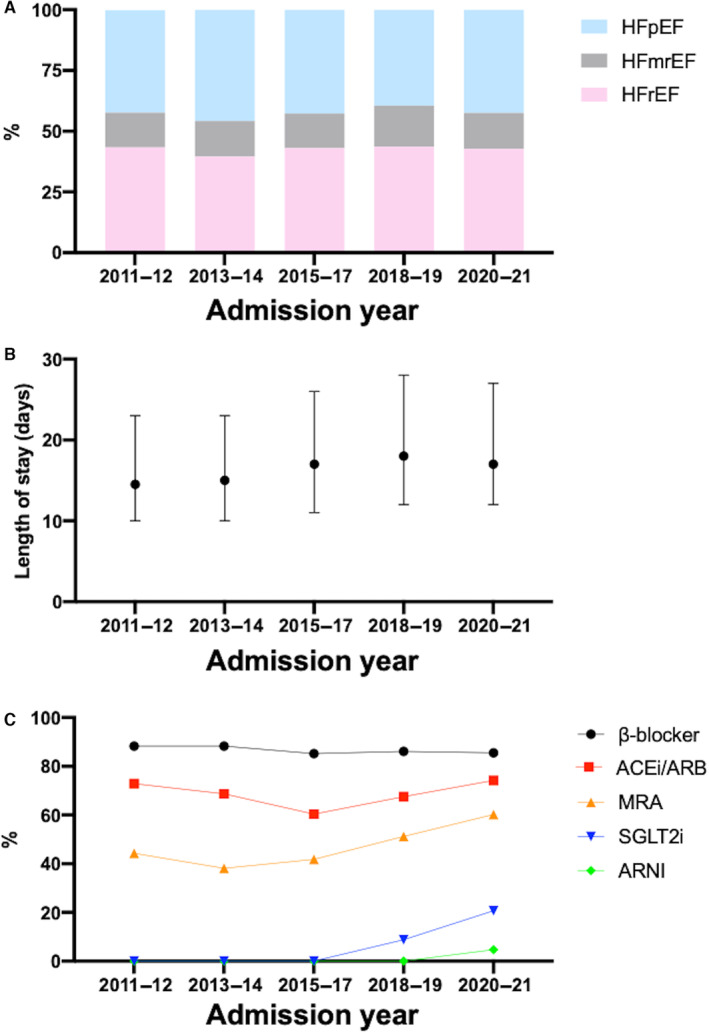
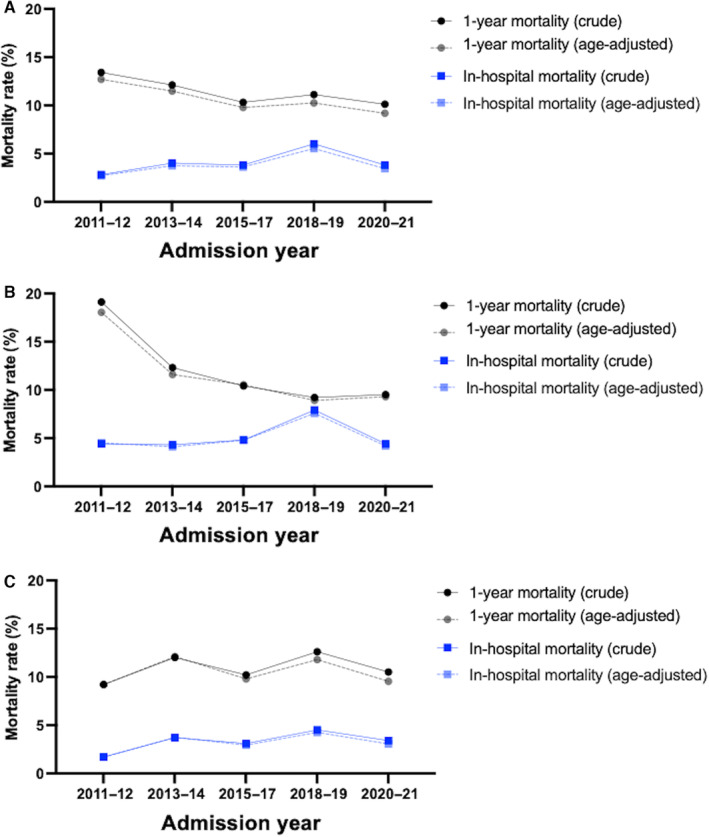
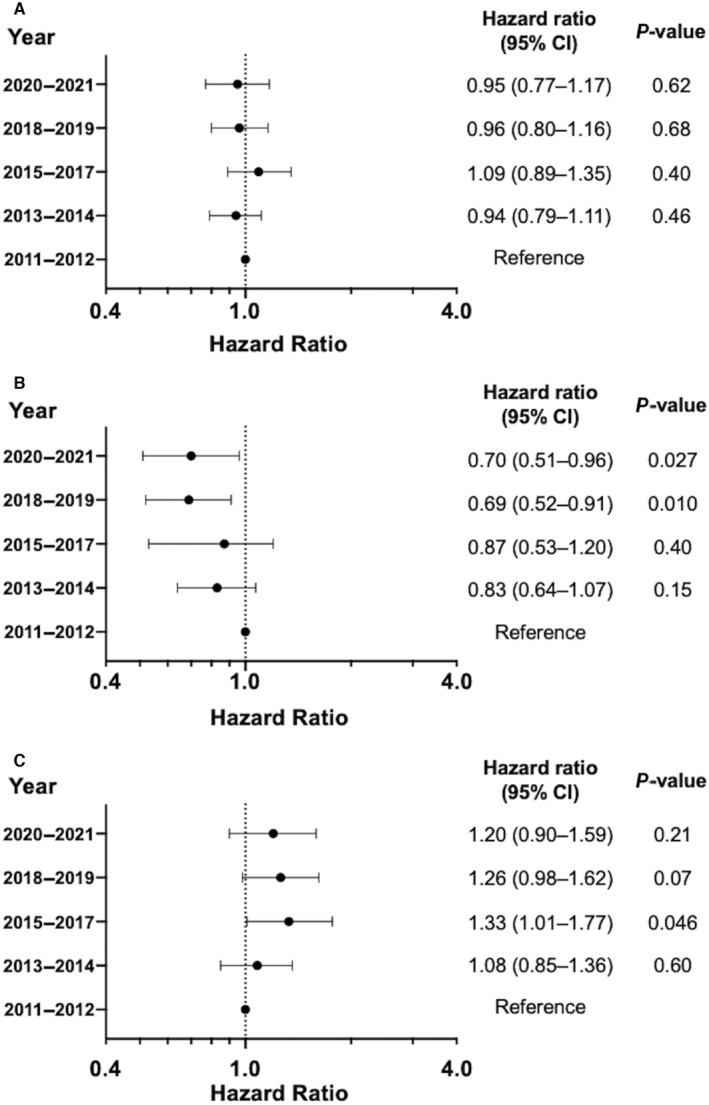
Background The management of heart failure (HF) has markedly changed, due to changes in demographics and the emergence of novel pharmacotherapies. However, detailed analyses on the temporal trends in characteristics and outcomes among patients with HF are scarcely available. This study aimed to assess the temporal trends over 11 years in clinical management and outcomes in patients with HF. Methods and Results We analyzed data from a multicenter registry of hospitalized patients with acute HF, including 6877 patients registered from 2011 to 2021. Age-adjusted mortality was calculated using standardized mortality ratios. During the study period, mean age increased from 75.2 years in 2011 to 2012 to 76.4 years in 2020 to 2021 (P for trend <0.001). The proportion of HF with reduced ejection fraction (HFrEF, left ventricular ejection fraction <40%) remained constant (from 43.4% to 42.7%, P for trend=0.38). The median duration of hospital stays (from 15 to 17 days, P for trend<0.001) had increased. As for the implementation of guideline-directed medical therapy, the use of mineralocorticoid receptor antagonist at discharge increased in patients with HFrEF (from 44.3% to 60.2%, P for trend<0.001). There was also an increase in the use of sodium-glucose cotransporter-2 inhibitors following their approval for use. The age-adjusted 1-year mortality decreased in patients with HFrEF (from 18.0% to 9.3%, P for trend<0.001) but not in patients with non-HFrEF (left ventricular ejection fraction ≥40%; from 9.2% to 9.5%, P for trend=0.79). Conclusions Hospitalized patients with HF have been aging over the past decade. Their long-term outcomes after discharge have improved predominantly because of decreased mortality in patients with HFrEF.
Keywords: acute heart failure; left ventricular ejection fraction; mortality; temporal trend.
Figures
References
-
- Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, Allison M, Hemingway H, Cleland JG, McMurray JJV, et al. Temporal trends and patterns in heart failure incidence: a population‐based study of 4 million individuals. Lancet. 2018;391:572–580. doi: 10.1016/S0140-6736(17)32520-5 - DOI - PMC - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e895–e1032. doi: 10.1161/CIR.0000000000001063 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
