

Population-level detection of early loss of kidney function: 7-year follow-up of a young adult cohort at risk of Mesoamerican nephropathy
- PMID: 37930052
- PMCID: PMC10859140
- DOI: 10.1093/ije/dyad151
Population-level detection of early loss of kidney function: 7-year follow-up of a young adult cohort at risk of Mesoamerican nephropathy
Erratum in
-
Correction to: Population-level detection of early loss of kidney function: 7-year follow-up of a young adult cohort at risk of Mesoamerican nephropathy.Int J Epidemiol. 2024 Feb 1;53(1):dyad163. doi: 10.1093/ije/dyad163. Int J Epidemiol. 2024. PMID: 38031436 Free PMC article. No abstract available.
Abstract
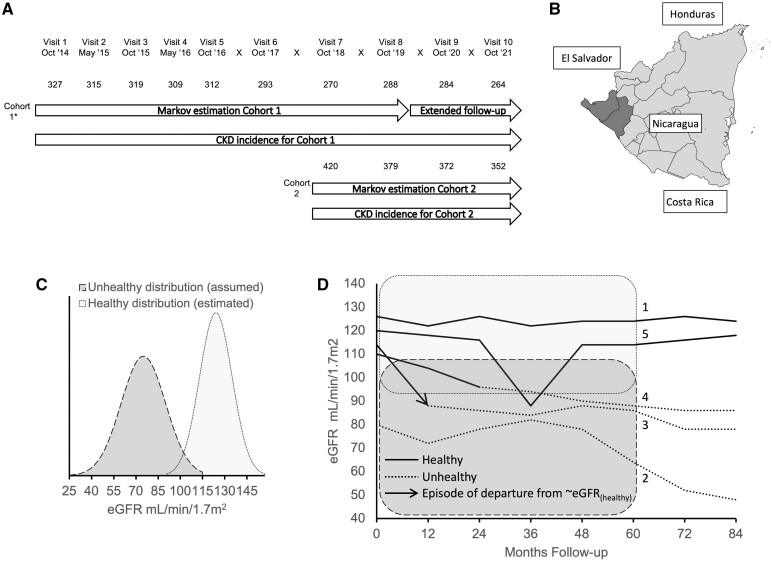
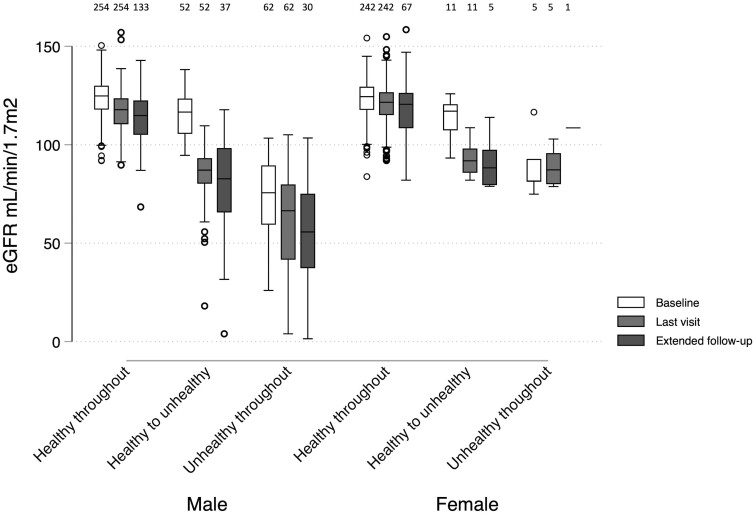
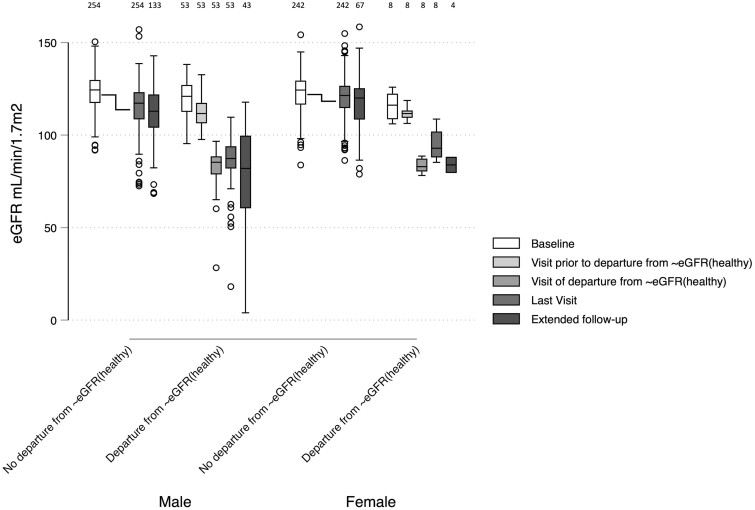
Background: Mesoamerican nephropathy is a leading contributor to premature mortality in Central America. Efforts to identify the cause are hampered by difficulties in distinguishing associations with potential initiating factors from common exposures thought to exacerbate the progression of all forms of established chronic kidney disease (CKD). We explored evidence of disease onset or departure from the healthy estimated glomerular filtration rate distribution [departure from ∼eGFR(healthy)] in an at-risk population.
Methods: Two community-based cohorts (adults aged 18-30 years, n = 351 and 420) from 11 rural communities in Northwest Nicaragua were followed up over 7 and 3 years respectively. We examined associations with both (i) incident CKD and (ii) the time point of departure from ∼eGFR(healthy), using a hidden Markov model.
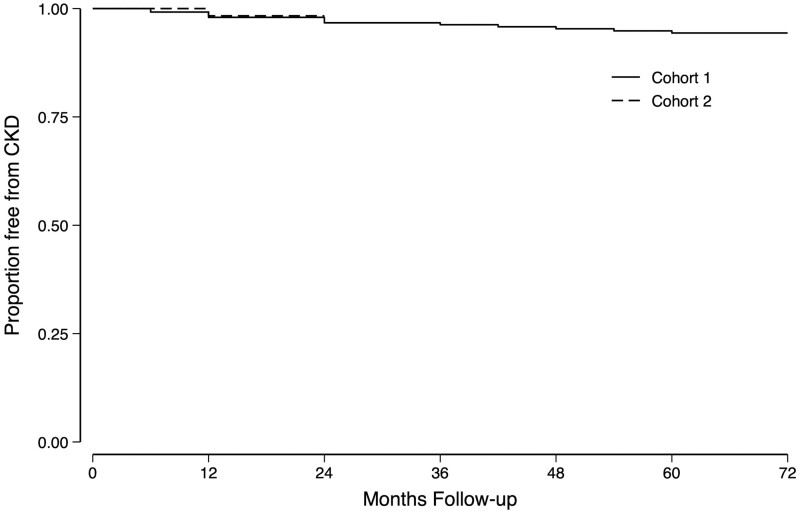
Results: CKD occurred in men only (male incidence rate: 0.7%/year). Fifty-three (out of 1878 visits, 2.7%) and 8 (out of 1067 visits, 0.8%) episodes of probable departure from ∼eGFR(healthy) occurred in men and women, respectively. Cumulative time in sugarcane work and symptoms of excess occupational sun exposure were associated with incident CKD. The same exposures were associated with probability of departure from ∼eGFR(healthy) in time-updated analyses along with measured and self-reported weight loss, nausea, vomiting and cramps, as well as non-steroidal anti-inflammatory drug use.
Conclusions: CKD burden in this population is high and risk factors for established disease are occupational. Additionally, a syndrome suggesting an alternative exposure is associated with evidence of disease onset supporting a possible separate unknown initiating factor for which further investigation is needed. Interventions to reduce the impact of occupational risks should be pursued meanwhile.
Keywords: Chronic kidney disease of undetermined cause; chronic kidney disease of non-traditional cause; hidden Markov modelling.
© The Author(s) 2023. Published by Oxford University Press on behalf of the International Epidemiological Association.
Conflict of interest statement
None declared.
Figures
References
-
- Caplin B, Yang CW, Anand S. et al. ; International Society of Nephrology’s International Consortium of Collaborators on Chronic Kidney Disease of Unknown Etiology (i3C). The International Society of Nephrology’s International Consortium of Collaborators on Chronic Kidney Disease of Unknown Etiology: report of the working group on approaches to population-level detection strategies and recommendations for a minimum dataset. Kidney Int 2019;95:4–10. - PubMed
-
- Cohen J. Mesoamerica’s mystery killer. Science 2014;344:143–47. - PubMed
-
- Kupferman J, Ramirez-Rubio O, Amador JJ. et al. Acute kidney injury in sugarcane workers at risk for Mesoamerican Nephropathy. Am J Kidney Dis 2018;72:475–82. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
