

Outcomes of cochlear implantation in Usher syndrome: a systematic review
- PMID: 37930386
- PMCID: PMC10858075
- DOI: 10.1007/s00405-023-08304-2
Outcomes of cochlear implantation in Usher syndrome: a systematic review
Abstract
Purpose: This study is a systematic review of the literature which seeks to evaluate auditory and quality of life (QOL) outcomes of cochlear implantation in patients with Usher syndrome.
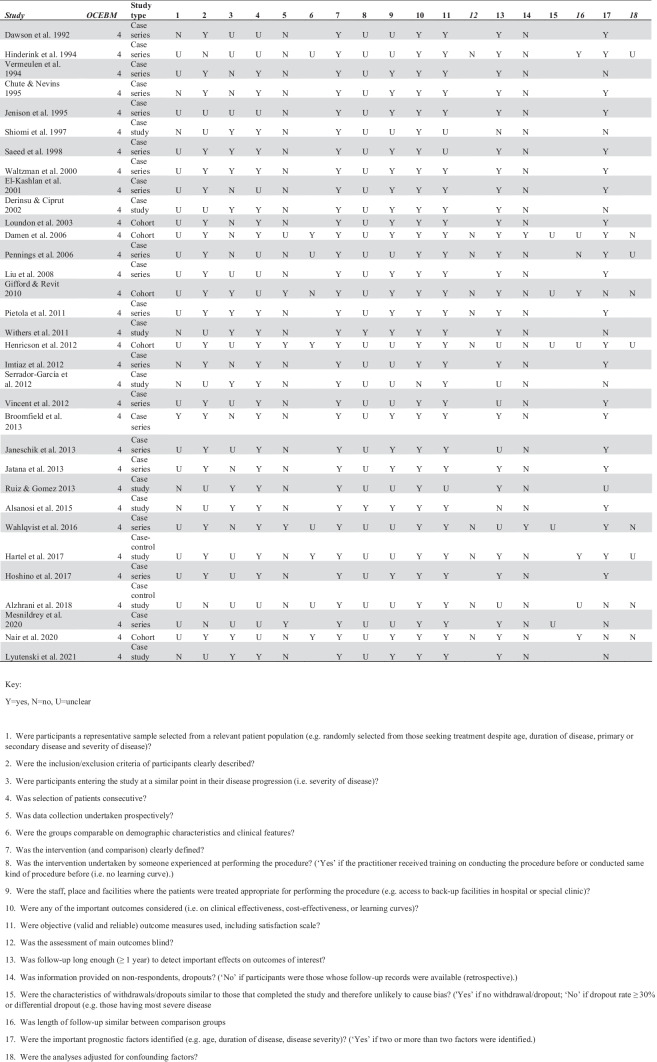
Methods: Systematic review of studies indexed in Medline via PubMed, Ovid EMBASE, Web of Science, CENTRAL and clinicaltrials.gov was performed up to March 9th 2022, conducted in accordance with the PRISMA statement. Patient demographics, comorbidity, details of cochlear implantation, auditory, and QOL outcomes were extracted and summarized.
Results: 33 studies reported over 217 cochlear implants in 187 patients with Usher syndrome, comprising subtypes 1 (56 patients), 2 (9 patients), 3 (23 patients), and not specified (99 patients). Auditory outcomes included improved sound detection, speech perception, and speech intelligibility. QOL outcomes were reported for 75 patients, with benefit reported in the majority.
Conclusions: Many patients with Usher syndrome develop improved auditory outcomes after cochlear implantation with early implantation being an important factor.
Keywords: Cochlear implant; Hearing loss; Quality of life; Usher syndrome.
© 2023. The Author(s).
Figures

References
-
- Lentz J, Keats BJB. Usher syndrome type I. In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K, Amemiya A, editors. GeneReviews®. Seattle, WA: University of Washington; 1993. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
