

Prescription Opioid Dose Reductions and Potential Adverse Events: a Multi-site Observational Cohort Study in Diverse US Health Systems
- PMID: 37930512
- PMCID: PMC11074095
- DOI: 10.1007/s11606-023-08459-y
Prescription Opioid Dose Reductions and Potential Adverse Events: a Multi-site Observational Cohort Study in Diverse US Health Systems
Abstract
Background: In response to the opioid crisis in the United States, population-level prescribing of opioids has been decreasing; there are concerns, however, that dose reductions are related to potential adverse events.
Objective: Examine associations between opioid dose reductions and risk of 1-month potential adverse events (emergency department (ED) visits, opioid overdose, benzodiazepine prescription fill, all-cause mortality).
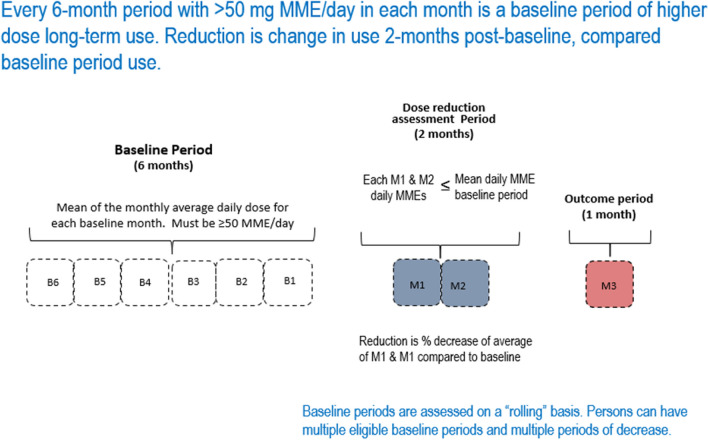
Design: This observational cohort study used electronic health record and claims data from eight United States health systems in a prescription opioid registry (Clinical Trials Network-0084). All opioid fills (excluding buprenorphine) between 1/1/2012 and 12/31/2018 were used to identify baseline periods with mean morphine milligram equivalents daily dose of ≥ 50 during six consecutive months.
Patients: We identified 60,040 non-cancer patients with ≥ one 2-month dose reduction period (600,234 unique dose reduction periods).
Main measures: Analyses examined associations between dose reduction levels (1- < 15%, 15- < 30%, 30- < 100%, 100% over 2 months) and potential adverse events in the month following a dose reduction using logistic regression analysis, adjusting for patient characteristics.
Key results: Overall, dose reduction periods involved mean reductions of 18.7%. Compared to reductions of 1- < 15%, dose reductions of 30- < 100% were associated with higher odds of ED visits (OR 1.14, 95% CI 1.10, 1.17), opioid overdose (OR 1.41, 95% CI 1.09-1.81), and all-cause mortality (OR 1.39, 95% CI 1.16-1.67), but lower odds of a benzodiazepine fill (OR 0.83, 95% CI 0.81-0.85). Dose reductions of 15- < 30%, compared to 1- < 15%, were associated with higher odds of ED visits (OR 1.08, 95% CI 1.05-1.11) and lower odds of a benzodiazepine fill (OR 0.93, 95% CI 0.92-0.95), but were not associated with opioid overdose and all-cause mortality.
Conclusions: Larger reductions for patients on opioid therapy may raise risk of potential adverse events in the month after reduction and should be carefully monitored.
Keywords: all-cause mortality; benzodiazepine prescription fill; emergency department visit; opioid dose reduction; opioid overdose.
© 2023. The Author(s), under exclusive licence to Society of General Internal Medicine.
Conflict of interest statement
Mr. Ray has received research support on grants to his institution in the past 3 years from Pfizer. Dr. Campbell, Dr. Hechter, and Mr. Ray have received research support to their institution from the Industry PMR Consortium, a consortium of companies working together to conduct post marketing studies required by the Food and Drug Administration that assesses risks related to opioid analgesic use. Dr. Andrade has received research support on grants to the University of Massachusetts Chan Medical School from Pfizer, Inc, and GlaxoSmithKline. Dr. Binswanger receives royalties from UpToDate (Wolters-Kluwer). The remaining authors report no conflict of interest (please see individual statements of each author). Ms. Rosa was substantially involved in the study, consistent with her role as Scientific Officer. She had no substantial involvement in the other cited grants.
References
-
- Drug overdose deaths in the U.S. top 100,000 annually. Centers for Disease Control and Prevention, National Center for Health Statistics. Last reviewed November 2021. Available at: https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2021/20211117.htm. Accessed September 26, 2023.
-
- Dahlhamer JM, Connor EM, Bose J, Lucas JL, Zelaya CE. Prescription opioid use among adults with chronic pain: United States, 2019. Natl Health Stat Report. 2021;162:1–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
