

Neurofilament Light Chain Elevation and Disability Progression in Multiple Sclerosis
- PMID: 37930670
- PMCID: PMC10628837
- DOI: 10.1001/jamaneurol.2023.3997
Neurofilament Light Chain Elevation and Disability Progression in Multiple Sclerosis
Abstract
Importance: Mechanisms contributing to disability accumulation in multiple sclerosis (MS) are poorly understood. Blood neurofilament light chain (NfL) level, a marker of neuroaxonal injury, correlates robustly with disease activity in people with MS (MS); however, data on the association between NfL level and disability accumulation have been conflicting.
Objective: To determine whether and when NfL levels are elevated in the context of confirmed disability worsening (CDW).
Design, setting, and participants: This study included 2 observational cohorts: results from the Expression, Proteomics, Imaging, Clinical (EPIC) study at the University of California San Francisco (since 2004) were confirmed in the Swiss Multiple Sclerosis Cohort (SMSC), a multicenter study in 8 centers since 2012. Data were extracted from EPIC in April 2022 (sampling July 1, 2004, to December 20, 2016) and SMSC in December 2022 (sampling June 6, 2012, to September 2, 2021). The study included 2 observational cohorts in tertiary MS centers. All participants of both cohorts with available NfL results were included in the study, and no eligible participants were excluded or declined to participate.
Exposure: Association between NfL z scores and CDW.
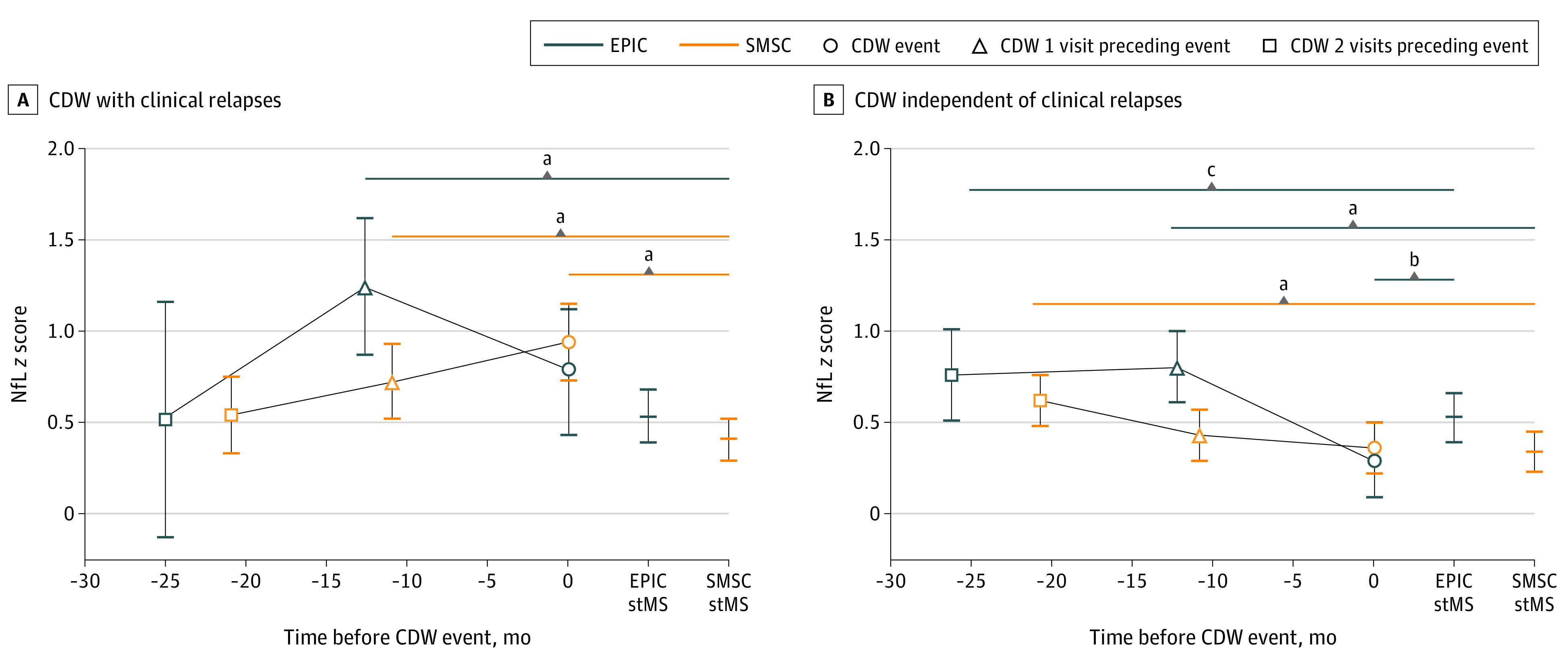
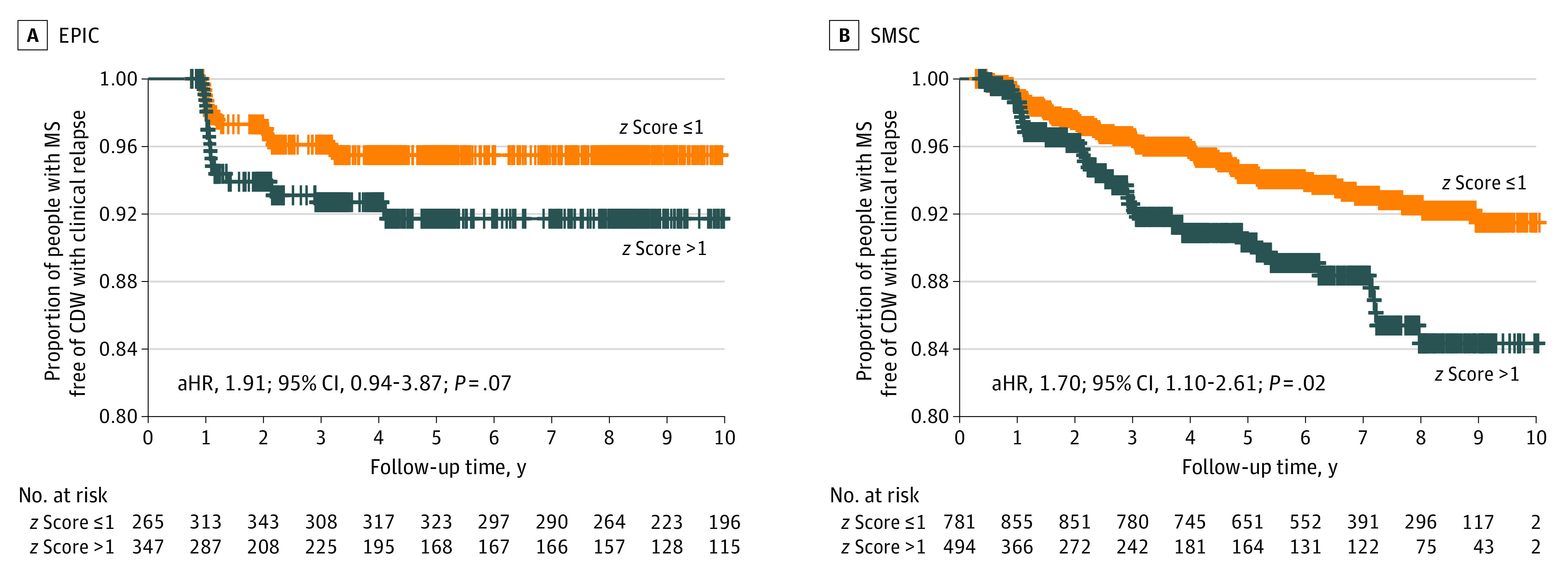
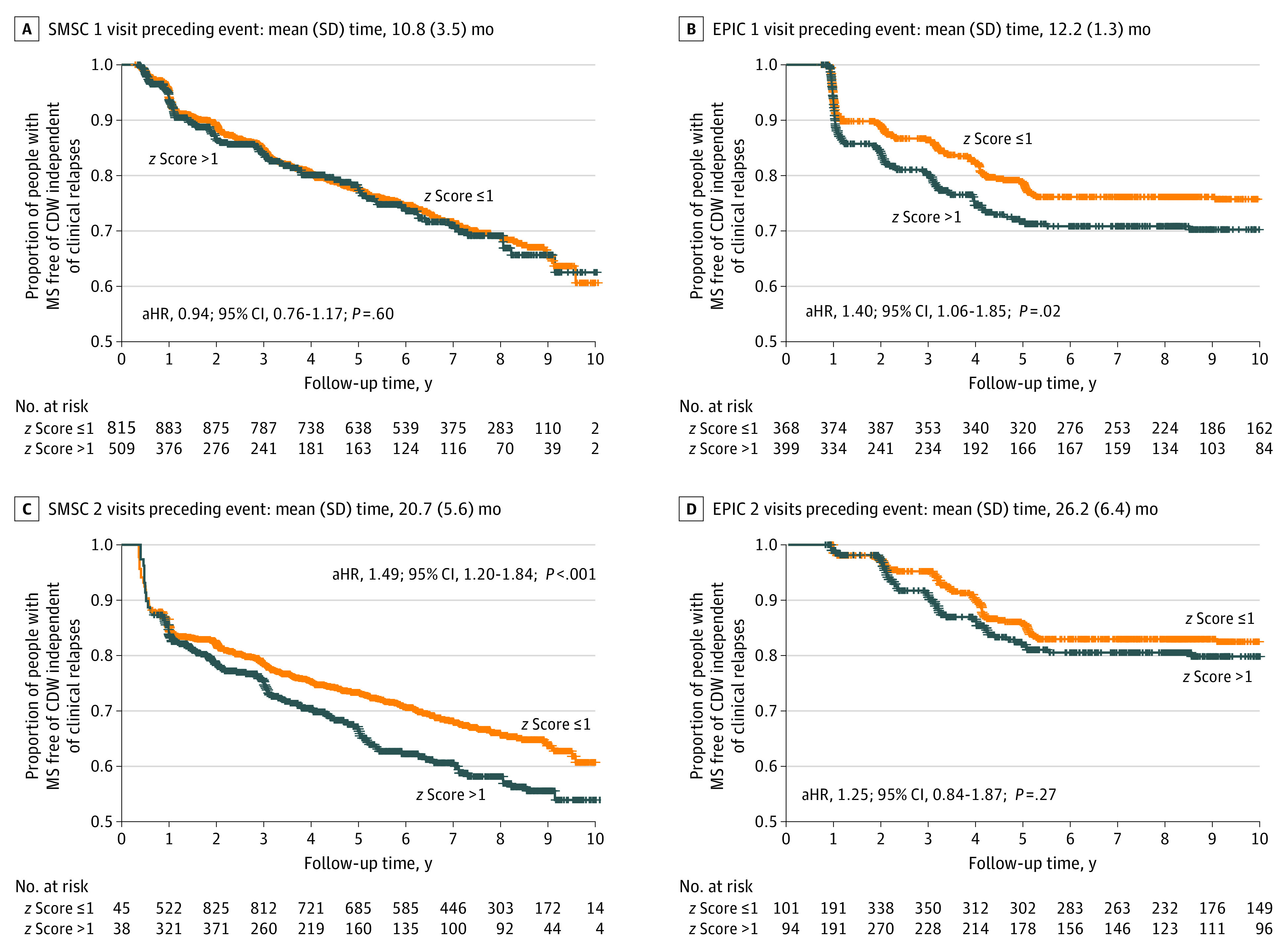
Main outcome measures: CDW was defined as Expanded Disability Status Scale (EDSS) worsening that was confirmed after 6 or more months and classified into CDW associated with clinical relapses (CDW-R) or independent of clinical relapses (CDW-NR). Visits were classified in relation to the disability worsening events into CDW(-2) for 2 visits preceding event, CDW(-1) for directly preceding event, CDW(event) for first diagnosis of EDSS increase, and the confirmation visit. Mixed linear and Cox regression models were used to evaluate NfL dynamics and to assess the association of NfL with future CDW, respectively.
Results: A total of 3906 EPIC visits (609 participants; median [IQR] age, 42.0 [35.0-50.0] years; 424 female [69.6%]) and 8901 SMSC visits (1290 participants; median [IQR] age, 41.2 [32.5-49.9] years; 850 female [65.9%]) were included. In CDW-R (EPIC, 36 events; SMSC, 93 events), NfL z scores were 0.71 (95% CI, 0.35-1.07; P < .001) units higher at CDW-R(-1) in EPIC and 0.32 (95% CI, 0.14-0.49; P < .001) in SMSC compared with stable MS samples. NfL elevation could be detected preceding CDW-NR (EPIC, 191 events; SMSC, 342 events) at CDW-NR(-2) (EPIC: 0.23; 95% CI, 0.01-0.45; P = .04; SMSC: 0.28; 95% CI, 0.18-0.37; P < .001) and at CDW-NR(-1) (EPIC: 0.27; 95% CI, 0.11-0.44; P < .001; SMSC: 0.09; 95% CI, 0-0.18; P = .06). Those findings were replicated in the subgroup with relapsing-remitting MS. Time-to-event analysis confirmed the association between NfL levels and future CDW-R within approximately 1 year and CDW-NR (in approximately 1-2 years).
Conclusions and relevance: This cohort study documents the occurrence of NfL elevation in advance of clinical worsening and may hint to a potential window of ongoing dynamic central nervous system pathology that precedes the diagnosis of CDW.
Conflict of interest statement
Figures
References
-
- Benkert P, Meier S, Schaedelin S, et al. ; NfL Reference Database in the Swiss Multiple Sclerosis Cohort Study Group . Serum neurofilament light chain for individual prognostication of disease activity in people with multiple sclerosis: a retrospective modelling and validation study. Lancet Neurol. 2022;21(3):246-257. doi:10.1016/S1474-4422(22)00009-6 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
