

Characterization of unipolar electrogram morphology: a novel tool for quantifying conduction inhomogeneity
- PMID: 37931071
- PMCID: PMC10657215
- DOI: 10.1093/europace/euad324
Characterization of unipolar electrogram morphology: a novel tool for quantifying conduction inhomogeneity
Abstract
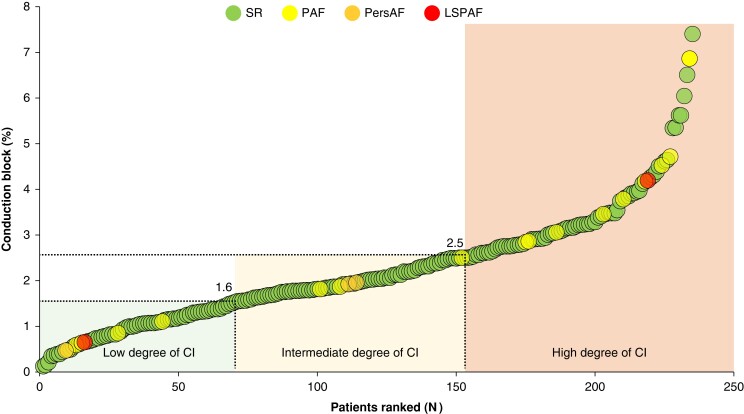
Aims: Areas of conduction inhomogeneity (CI) during sinus rhythm may facilitate the initiation and perpetuation of atrial fibrillation (AF). Currently, no tool is available to quantify the severity of CI. Our aim is to develop and validate a novel tool using unipolar electrograms (EGMs) only to quantify the severity of CI in the atria.
Methods and results: Epicardial mapping of the right atrium (RA) and left atrium, including Bachmann's bundle, was performed in 235 patients undergoing coronary artery bypass grafting surgery. Conduction inhomogeneity was defined as the amount of conduction block. Electrograms were classified as single, short, long double (LDP), and fractionated potentials (FPs), and the fractionation duration of non-single potentials was measured. The proportion of low-voltage areas (LVAs, <1 mV) was calculated. Increased CI was associated with decreased potential voltages and increased LVAs, LDPs, and FPs. The Electrical Fingerprint Score consisting of RA EGM features, including LVAs and LDPs, was most accurate in predicting CI severity. The RA Electrical Fingerprint Score demonstrated the highest correlation with the amount of CI in both atria (r = 0.70, P < 0.001).
Conclusion: The Electrical Fingerprint Score is a novel tool to quantify the severity of CI using only unipolar EGM characteristics recorded. This tool can be used to stage the degree of conduction abnormalities without constructing spatial activation patterns, potentially enabling early identification of patients at high risk of post-operative AF or selection of the appropriate ablation approach in addition to pulmonary vein isolation at the electrophysiology laboratory.
Keywords: Atrial fibrillation; Conduction inhomogeneity; Diagnostic tool; Epicardial mapping; Sinus rhythm.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures








References
-
- Allessie MA, de Groot NMS, Houben RPM, Schotten U, Boersma E, Smeets JLet al. Electropathological substrate of long-standing persistent atrial fibrillation in patients with structural heart disease: longitudinal dissociation. Circ Arrhythm Electrophysiol 2010;3:606–15. - PubMed
-
- Pytkowski M, Jankowska A, Maciag A, Kowalik I, Sterlinski M, Szwed Het al. Paroxysmal atrial fibrillation is associated with increased intra-atrial conduction delay. Europace 2008;10:1415–20. - PubMed
-
- de Groot NM, Schalij MJ, Zeppenfeld K, Blom NA, Van der Velde ET, Van der Wall EE. Voltage and activation mapping: how the recording technique affects the outcome of catheter ablation procedures in patients with congenital heart disease. Circulation 2003;108:2099–106. - PubMed
-
- Miyamoto K, Tsuchiya T, Narita S, Yamaguchi T, Nagamoto Y, Ando Set al. Bipolar electrogram amplitudes in the left atrium are related to local conduction velocity in patients with atrial fibrillation. Europace 2009;11:1597–605. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
