

Standard Versus Modified Ipilimumab, in Combination With Nivolumab, in Advanced Renal Cell Carcinoma: A Randomized Phase II Trial (PRISM)
- PMID: 37931206
- PMCID: PMC10824383
- DOI: 10.1200/JCO.23.00236
Standard Versus Modified Ipilimumab, in Combination With Nivolumab, in Advanced Renal Cell Carcinoma: A Randomized Phase II Trial (PRISM)
Abstract
Purpose: Ipilimumab (IPI), in combination with nivolumab (NIVO), is an approved frontline treatment option for patients with intermediate- or poor-risk advanced renal cell carcinoma (aRCC). We conducted a randomized phase II trial to evaluate whether administering IPI once every 12 weeks (modified), instead of once every 3 weeks (standard), in combination with NIVO, is associated with a favorable toxicity profile.
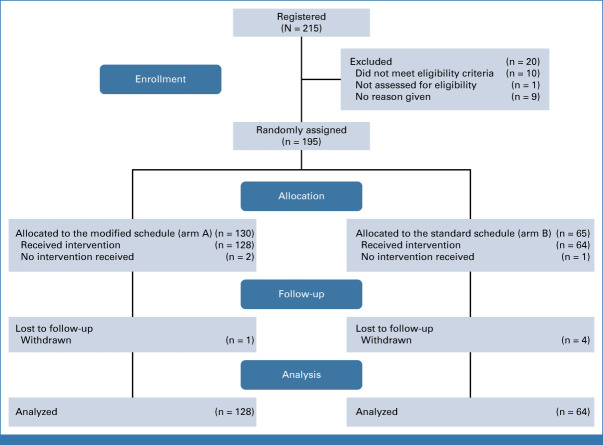
Methods: Treatment-naïve patients with clear-cell aRCC were randomly assigned 2:1 to receive four doses of modified or standard IPI, 1 mg/kg, in combination with NIVO (3 mg/kg). The primary end point was the proportion of patients with a grade 3-5 treatment-related adverse event (trAE) among those who received at least one dose of therapy. The key secondary end point was 12-month progression-free survival (PFS) in the modified arm compared with historical sunitinib control. The study was not designed to formally compare arms for efficacy.
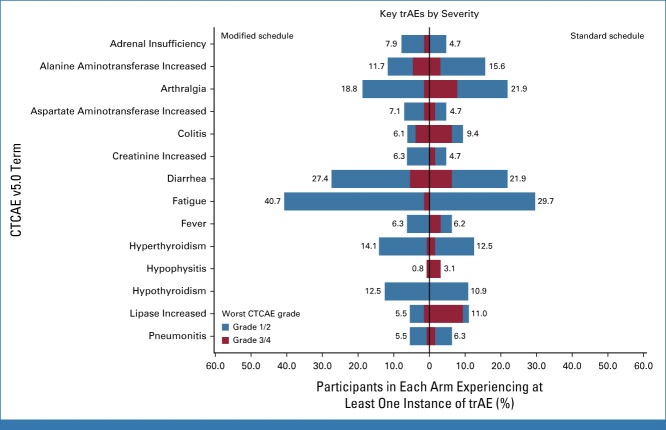
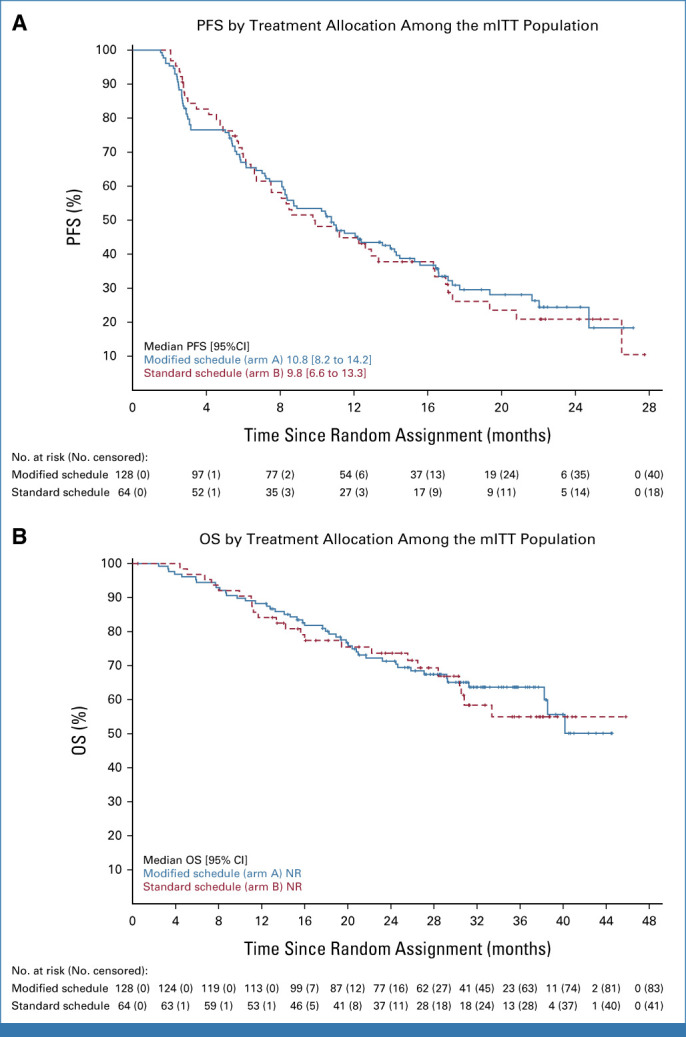
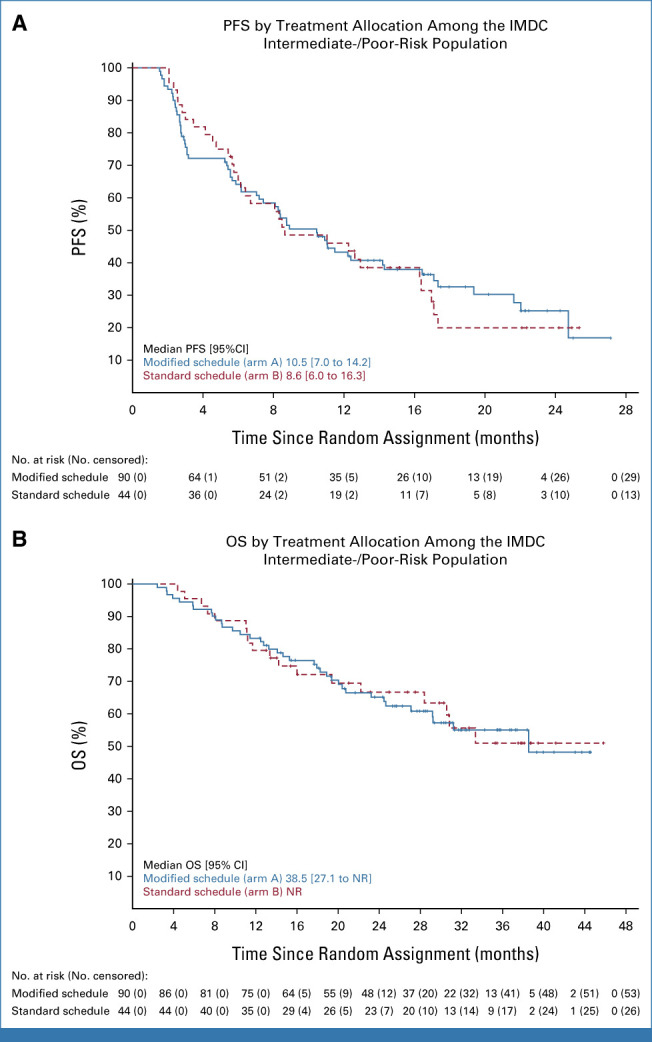
Results: Between March 2018 and January 2020, 192 patients (69.8% intermediate/poor-risk) were randomly assigned and received at least one dose of study drug. The incidence of grade 3-5 trAEs was significantly lower among participants receiving modified versus standard IPI (32.8% v 53.1%; odds ratio, 0.43 [90% CI, 0.25 to 0.72]; P = .0075). The 12-month PFS (90% CI) using modified IPI was 46.1% (38.6 to 53.2). At a median follow-up of 21 months, the overall response rate was 45.3% versus 35.9% and the median PFS was 10.8 months versus 9.8 months in the modified and standard IPI groups, respectively.
Conclusion: Rates of grade 3-5 trAEs were significantly lower in patients receiving modified versus standard IPI. Although 12-month PFS did not meet the prespecified efficacy threshold compared with historical control, informal comparison of treatment groups did not suggest any reduction in efficacy with the modified schedule.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO’s conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures
References
-
- Heng DYC, Xie W, Regan MM, et al. : Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: Results from a large, multicenter study. J Clin Oncol 27:5794-5799, 2009 - PubMed
-
- Motzer RJ, Escudier B, McDermott DF, et al. : Survival outcomes and independent response assessment with nivolumab plus ipilimumab versus sunitinib in patients with advanced renal cell carcinoma: 42-month follow-up of a randomized phase 3 clinical trial. J Immunother Cancer 8:e000891, 2020 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
