

Causes and consequences of clonal hematopoiesis
- PMID: 37931207
- PMCID: PMC10862247
- DOI: 10.1182/blood.2023022222
Causes and consequences of clonal hematopoiesis
Abstract
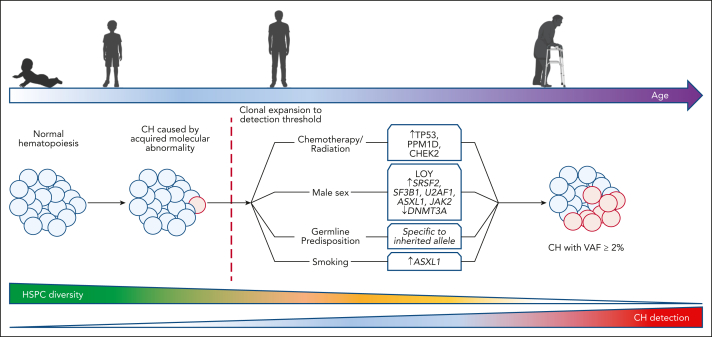
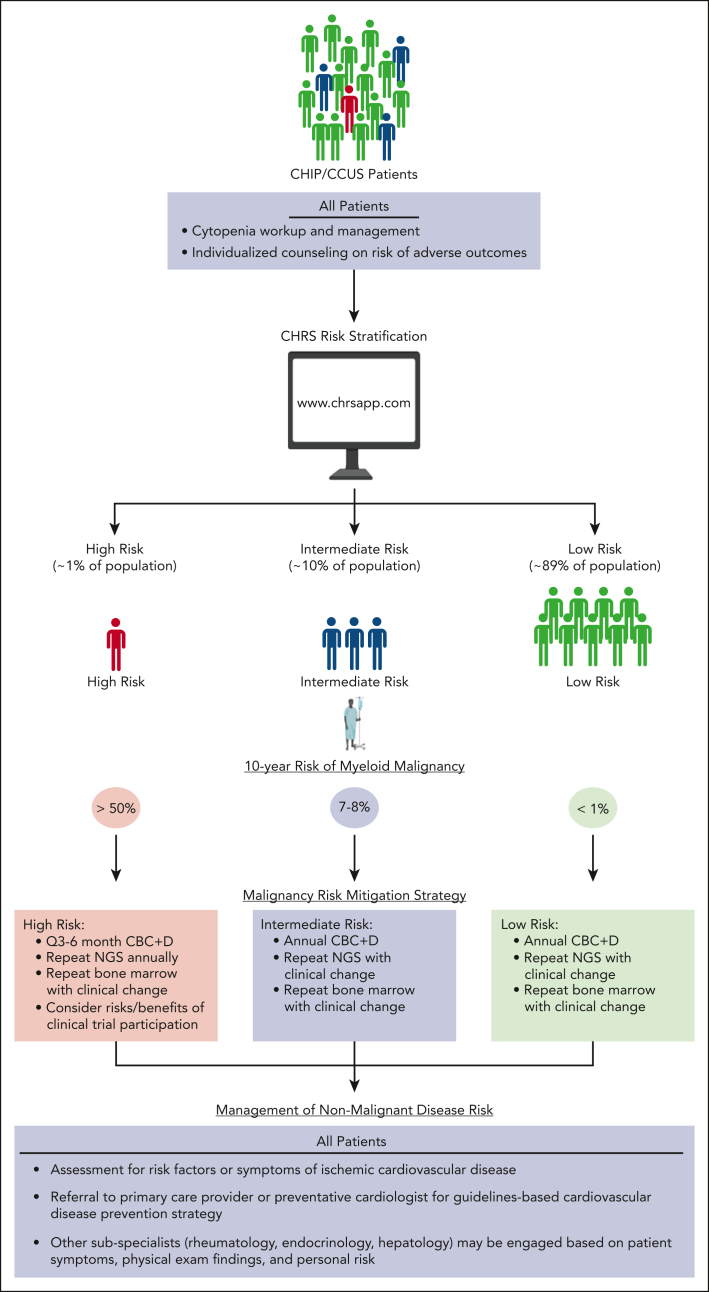
Clonal hematopoiesis (CH) is described as the outsized contribution of expanded clones of hematopoietic stem and progenitor cells (HSPCs) to blood cell production. The prevalence of CH increases dramatically with age. CH can be caused by somatic mutations in individual genes or by gains and/or losses of larger chromosomal segments. CH is a premalignant state; the somatic mutations detected in CH are the initiating mutations for hematologic malignancies, and CH is a strong predictor of the development of blood cancers. Moreover, CH is associated with nonmalignant disorders and increased overall mortality. The somatic mutations that drive clonal expansion of HSPCs can alter the function of terminally differentiated blood cells, including the release of elevated levels of inflammatory cytokines. These cytokines may then contribute to a broad range of inflammatory disorders that increase in prevalence with age. Specific somatic mutations in the peripheral blood in coordination with blood count parameters can powerfully predict the development of hematologic malignancies and overall mortality in CH. In this review, we summarize the current understanding of CH nosology and origins. We provide an overview of available tools for risk stratification and discuss management strategies for patients with CH presenting to hematology clinics.
© 2023 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: B.L.E. has received research funding from Celgene, Deerfield, and Novartis and consulting fees from GRAIL; and serves on the scientific advisory boards for Skyhawk Therapeutics, Exo Therapeutics, Neomorph, and TenSixteen Bio, all unrelated to this work. L.D.W. has received consulting fees from AbbVie, Vertex, and Sobi, all unrelated to this work.
Figures




Comment in
-
Diagnosis and classification of myelodysplastic syndromes.Blood. 2023 Dec 28;142(26):2247-2257. doi: 10.1182/blood.2023020078. Blood. 2023. PMID: 37774372
-
Clinical decision-making and treatment of myelodysplastic syndromes.Blood. 2023 Dec 28;142(26):2268-2281. doi: 10.1182/blood.2023020079. Blood. 2023. PMID: 37874917
References
-
- Kakiuchi N, Ogawa S. Clonal expansion in non-cancer tissues. Nat Rev Cancer. 2021;21(4):239–256. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
