

Distal femoral fractures in children
- PMID: 37931413
- PMCID: PMC9069856
- DOI: 10.1530/EOR-21-0110
Distal femoral fractures in children
Abstract
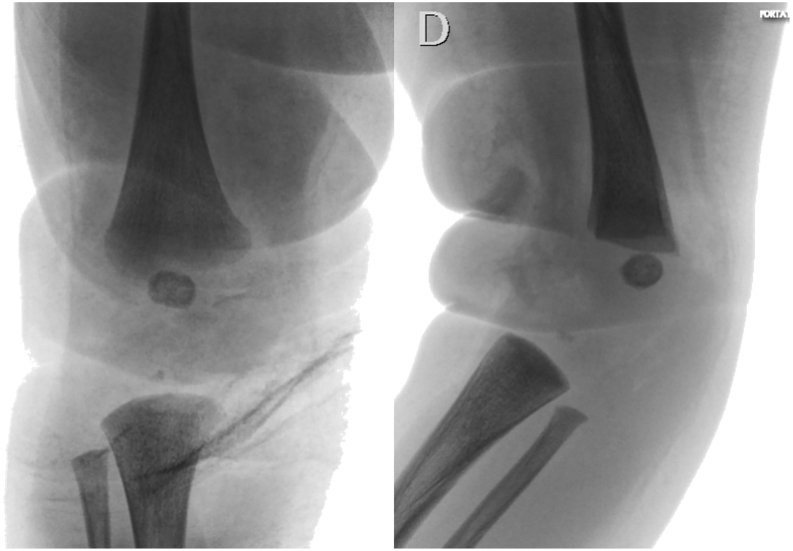
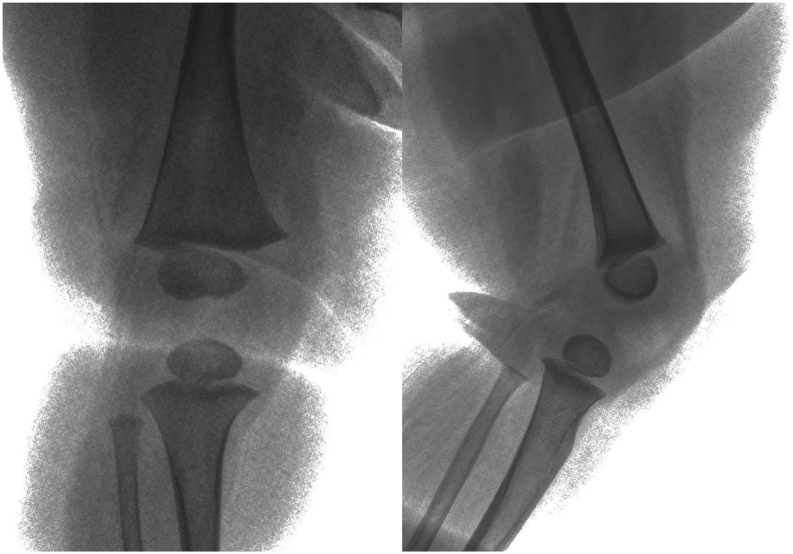
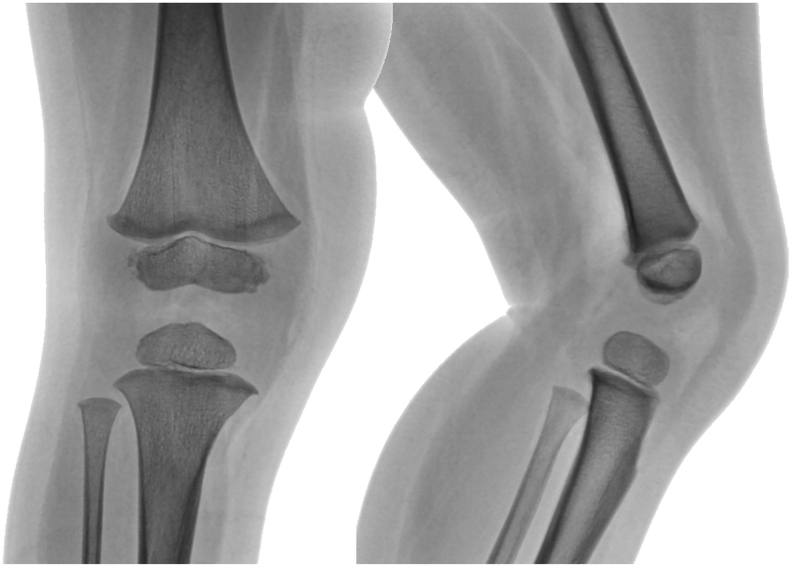
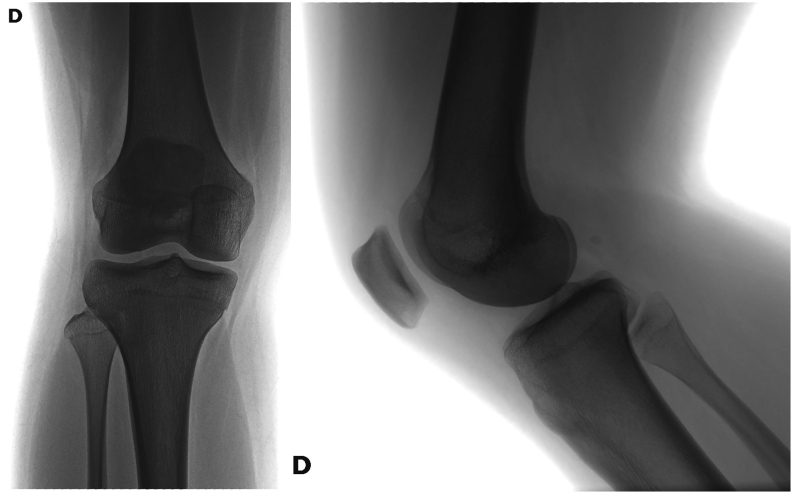
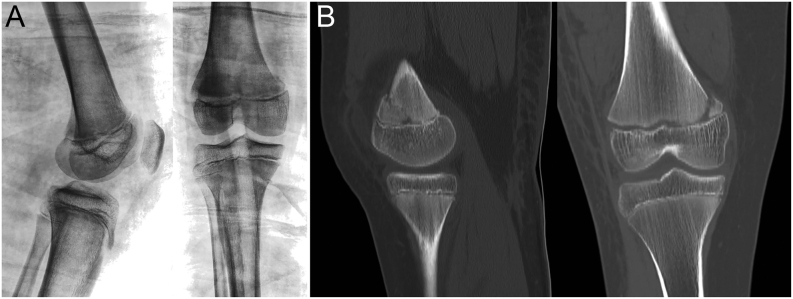
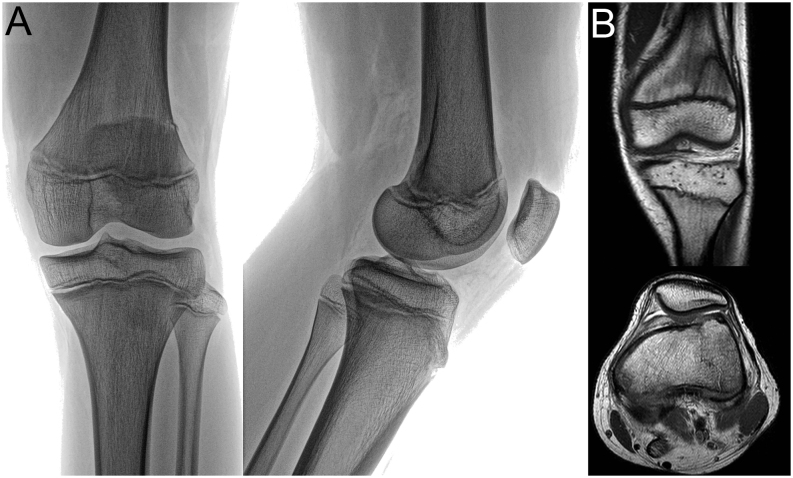
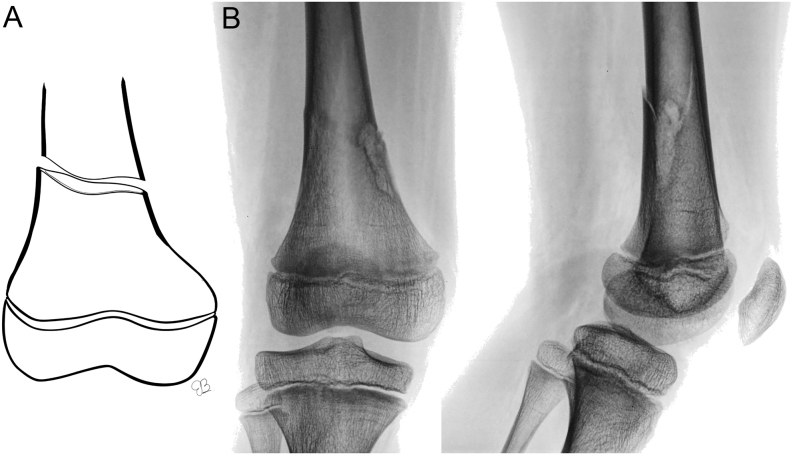
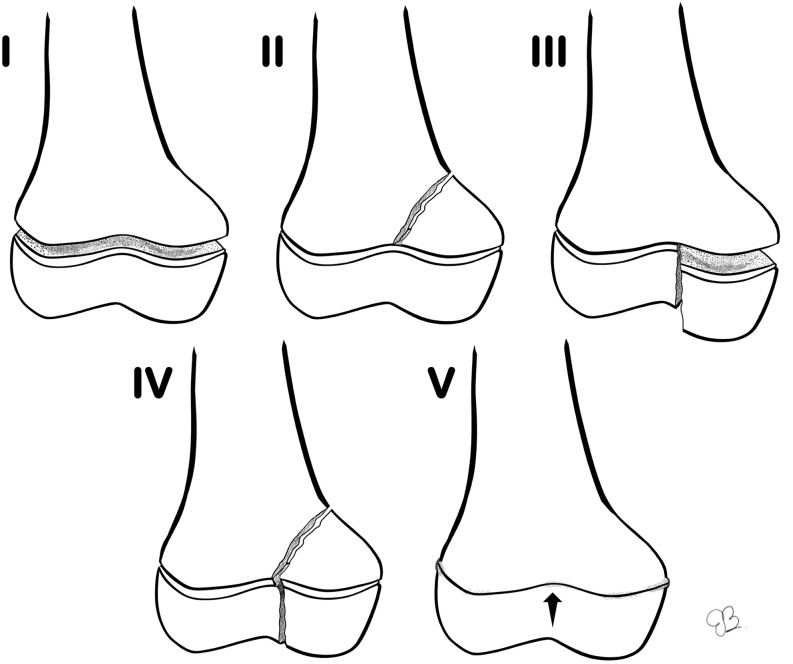
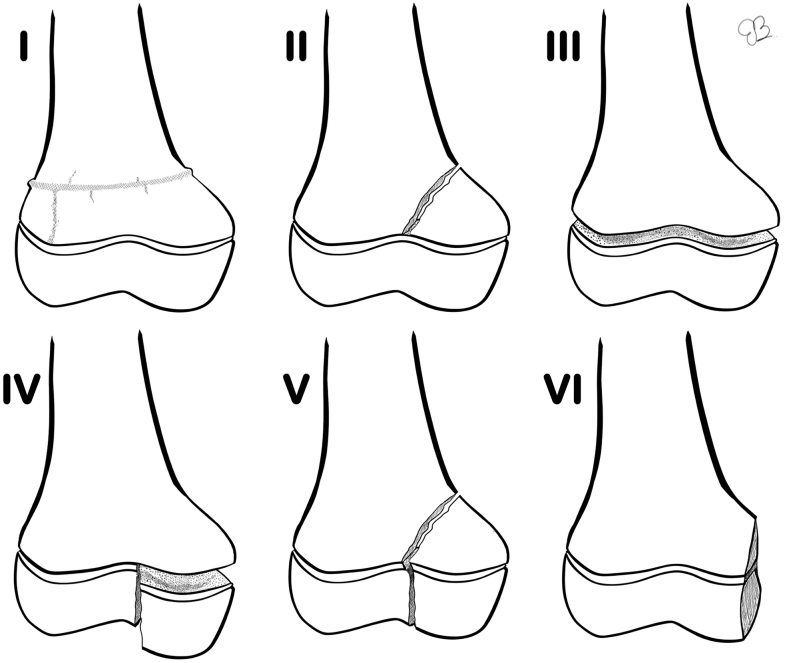
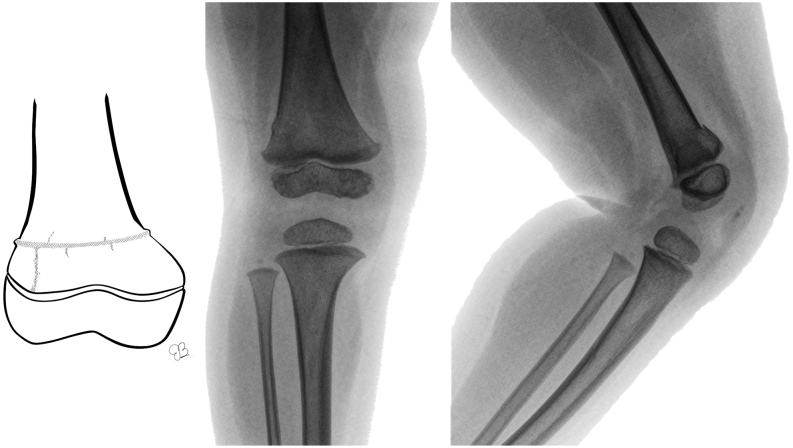
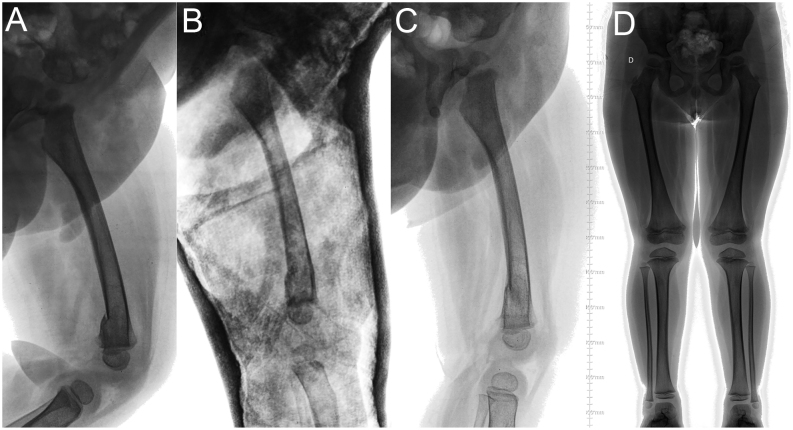
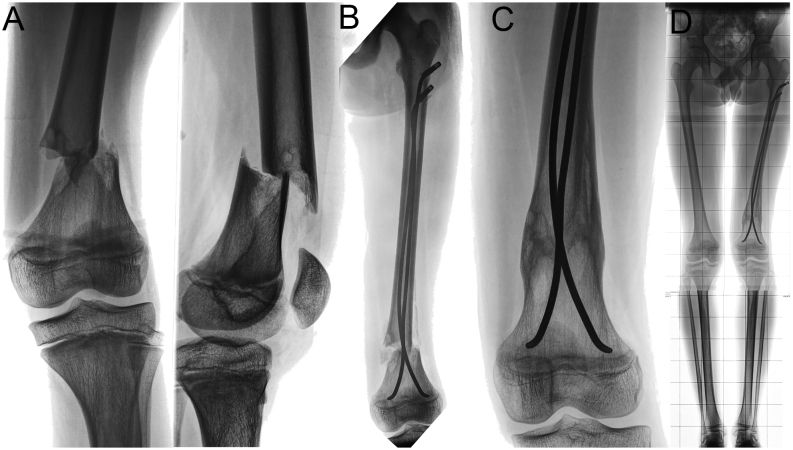
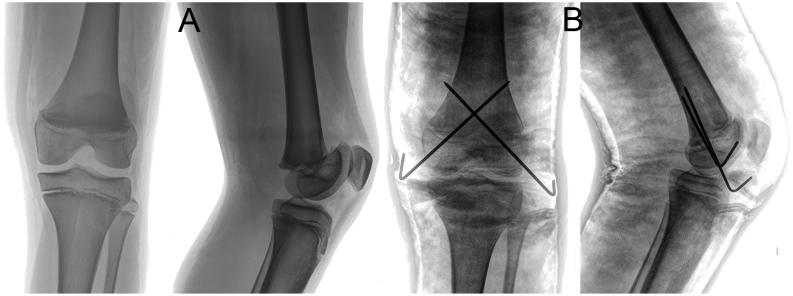
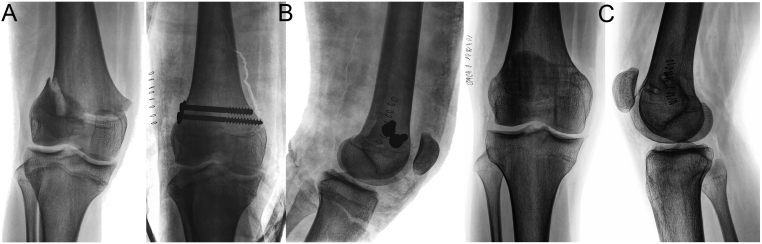
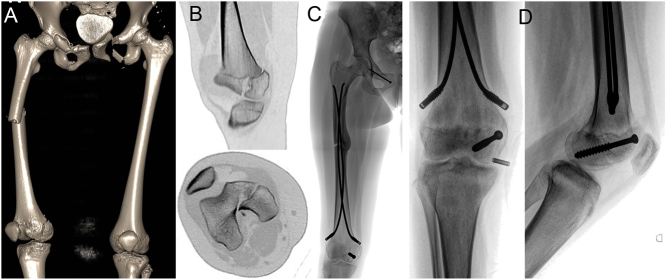
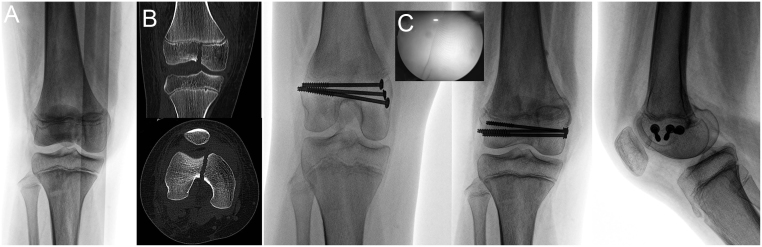
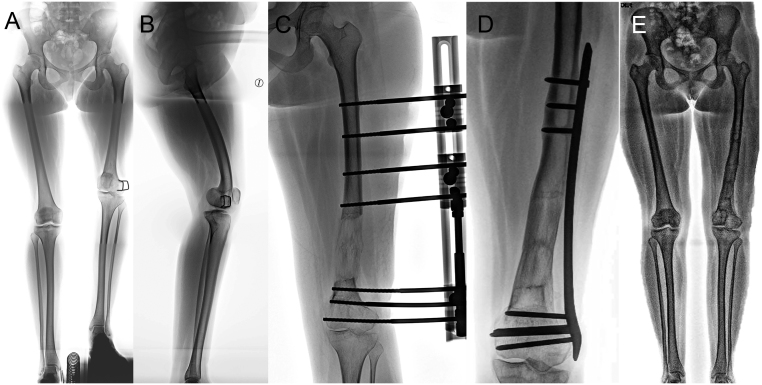
The physis of the distal femur contributes to 70% of femoral growth and 37% of the total limb growth; therefore, physeal injury can lead to important alterations of axes and length. Distal metaphyseal corner-type fracture prior to walking is classically associated with child abuse. In children aged >10 years, sports-related fractures and car accidents are significant contributors. Imaging includes a two-plane radiographic study of the knee. It is recommended to obtain radiographs that include the entire femur to rule out concomitant injuries. In cases of high suspicion of distal metaphyseal fractures and no radiographic evidence, CT or MRI can show the existence of hidden fractures. Fractures with physeal involvement are conventionally classified according to the Salter-Harris classification, but the Peterson classification is also recommended as it includes special subgroups. Conservative and surgical management are valid alternatives for the treatment of these fractures. Choosing between both alternatives depends on factors related to the fracture type. As there is a high risk of permanent physeal damage, long-term follow-up is essential until skeletal maturity is complete.
Keywords: femur; paediatrics; surgery; trauma.
Figures


References
-
- Salter RB, Harris WR. Injuries involving the epiphyseal plate. Journal of Bone and Joint Surgery 196345587–622. (10.2106/00004623-196345030-00019) - DOI
-
- Alhammoud A, Younis MH, Ahmed AF, Ibrahim T. Surgical versus nonsurgical treatment of distal femur physeal fractures: a systematic review and meta-analysis. Journal of Musculoskeletal Surgery and Research 20193179–183. (10.4103/jmsr.jmsr_53_18) - DOI
-
- Peterson HA.Part 2. Physeal fractures: anatomic sites. Chapter 18. Distal femur. In Epiphyseal Growth Plate Fractures, pp. 595–640. Berlin, Heidelberg: Springer-Verlag, 2007. (10.1007/978-3-540-33802-4) - DOI
-
- Ogden J.Chapter 21: Femur. In Skeletal Injury in the Child, 3rded., pp.857–928. New York: Springer-Verlag, 2000. (10.1007/b97655) - DOI
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
