

Lung Structure and Risk of Sleep Apnea in SPIROMICS
- PMID: 37931592
- PMCID: PMC10913931
- DOI: 10.15326/jcopdf.2023.0411
Lung Structure and Risk of Sleep Apnea in SPIROMICS
Abstract
Rationale: The SubPopulations and InteRmediate Outcome Measures in COPD Study (SPIROMICS) is a prospective cohort study that enrolled 2981 participants with the goal of identifying new chronic obstructive pulmonary disease (COPD) subgroups and intermediate markers of disease progression. Individuals with COPD and obstructive sleep apnea (OSA) experience impaired quality of life and more frequent exacerbations. COPD severity also associates with computed tomography scan-based emphysema and alterations in airway dimensions.
Objectives: The objective was to determine whether the combination of lung function and structure influences the risk of OSA among current and former smokers.
Methods: Using 2 OSA risk scores, the Berlin Sleep Questionnaire (BSQ), and the DOISNORE50 (Diseases, Observed apnea, Insomnia, Snoring, Neck circumference > 18 inches, Obesity with body mass index [BMI] > 32, R = are you male, Excessive daytime sleepiness, 50 = age ≥ 50) (DIS), 1767 current and former smokers were evaluated for an association of lung structure and function with OSA risk.
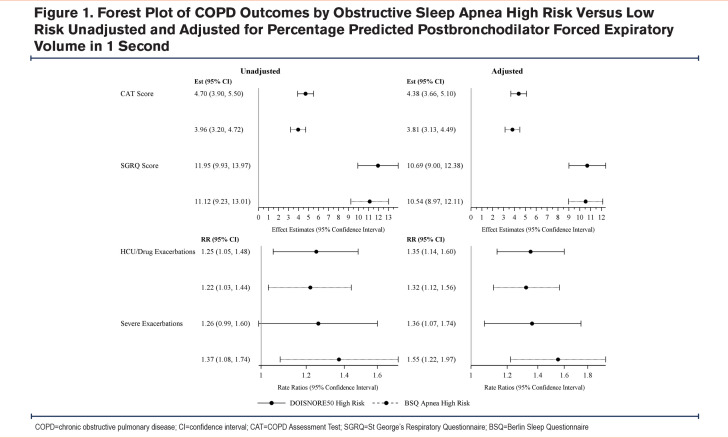
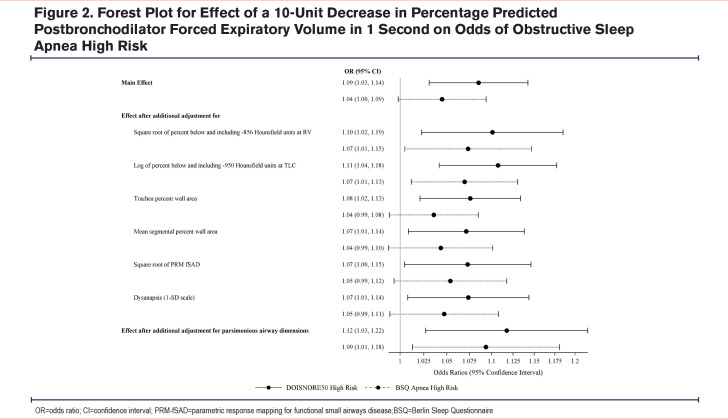
Measurements and main results: The study cohort's mean age was 63 years, BMI was 28 kg/m2, and forced expiratory volume in 1 second (FEV1) was 74.8% predicted. The majority were male (55%), White (77%), former smokers (59%), and had COPD (63%). A high-risk OSA score was reported in 36% and 61% using DIS and BSQ respectively. There was a 9% increased odds of a high-risk DIS score (odds ratio [OR]=1.09, 95% confidence interval [CI]:1.03-1.14) and nominally increased odds of a high-risk BSQ score for every 10% decrease in FEV1 %predicted (OR=1.04, 95%CI: 0.998-1.09). Lung function-OSA risk associations persisted after additionally adjusting for lung structure measurements (%emphysema, %air trapping, parametric response mapping for functional small airways disease, , mean segmental wall area, tracheal %wall area, dysanapsis) for DIS (OR=1.12, 95%CI:1.03-1.22) and BSQ (OR=1.09, 95%CI:1.01-1.18).
Conclusions: Lower lung function independently associates with having high risk for OSA in current and former smokers. Lung structural elements, especially dysanapsis, functional small airways disease, and tracheal %wall area strengthened the effects on OSA risk.
Keywords: COPD; CT-scan measurements; DOISNORE50; lung function.
JCOPDF © 2024.
Conflict of interest statement
Drs. Koch, Namen, Baugh, Sada, Zeidler, Comellas, Bowler, and Kanner and Ms. Shing have nothing to declare. Dr. Couper reports grants from the National Heart, Lung, and Blood Institute (NHLBI) and the COPD Foundation during the conduct of the study. Dr. Smith reports grants from the National Institutes of Health (NIH), the Canadian Institutes of Health Research, McGill University Health Centre Foundation, the Canadian Lung Association, and the Quebec Health Research Fund. Dr. Barr reports grants from the NIH, the Foundation for the NIH, and the COPD Foundation, during the conduct of the study; and grants from the Alpha-1 Foundation and personal fees from UpToDate, outside the submitted work. Dr. Bhatt reports grants from the NIH, has received consulting fees from Boehringer Ingelheim and Sanofi/Regeneron, and CME fees from Integrity CE in the past 3 years. Dr. Putcha reports grants from the NIH. Dr. Cooper reports grants from the NIH/NHLBI and the Foundation of the NIH, during the conduct of the study; personal fees from PulmonX and NUVAIRA, other from GlaxoSmithKline and personal fees from MGC Diagnostics, outside the submitted work. Dr. Barjaktarevic reports personal fees from AstraZeneca, personal fees from Boehringer Ingelheim, grants from AMGEN, grants and personal fees from GE Healthcare, personal fees from Grifols, personal fees from Verona Pharma, personal fees from GSK, grants and personal fees from Mylan/Theravance, outside the submitted work. Dr. Han reports personal fees from GSK, personal fees from BI, personal fees from AZ, personal fees from Merck, personal fees from Mylan, nonfinancial support from Novartis, and nonfinancial support from Sunovion, outside the submitted work. Dr. Kim reports personal fees from Galvanize Therapeutics for his role as a consultant (total sum <$5000). Dr. Paine reports grants from the NHLBI and the COPD Foundation, during the conduct of the study and grants from Department of Veterans Affairs, outside the submitted work. Dr. Krishnan reports research support from the NIH, the COPD Foundation, Regeneron, the Sergey Brin Family Foundation, the U.S Patient-Centered Outcomes Research Institute, and the American Lung Association and consulting fees paid by GSK (for COVID-19 biologics), AstraZeneca (for asthma biologics), CereVu Medical, Propeller/ResMed, and BData. Dr. Martinez reports grants from the Department of Defense, during the conduct of the study; personal fees, nonfinancial support, and other from AstraZeneca, personal fees, nonfinancial support, and other from Boehringer Ingelheim, nonfinancial support and other from ProterrixBio, personal fees from Columbia University, personal fees and nonfinancial support from Genentech, personal fees and nonfinancial support from GlaxoSmithKline, personal fees and nonfinancial support from Inova Fairfax Health System, personal fees from MD Magazine, personal fees from Methodist Hospital Brooklyn, personal fees and nonfinancial support from Miller Communications, personal fees and nonfinancial support from the National Association for Continuing Education, personal fees and nonfinancial support from Novartis, personal fees from New York University, personal fees and nonfinancial support from Pearl Pharmaceuticals, personal fees and nonfinancial support from PeerView Communications, personal fees and nonfinancial support from Prime Communications, personal fees and nonfinancial support from the Puerto Rican Respiratory Society, personal fees and nonfinancial support from Chiesi, personal fees and non-financial support from Sunovion, personal fees and nonfinancial support from Theravance, personal fees from UpToDate, personal fees from WebMD/MedScape, other from Afferent/Merck, nonfinancial support from Gilead, nonfinancial support from Nitto, personal fees and other from Patara/Respivant, personal fees and nonfinancial support from Potomac, other from Biogen, personal fees and nonfinancial support from the University of Alabama Birmingham, other from Veracyte, nonfinancial support from Zambon, personal fees from the American Thoracic Society, grants from NIH, personal fees and nonfinancial support from Physicians Education Resource, personal fees from Rockpointe, other from Prometic, personal fees from Rare Disease Healthcare Communications, other from Bayer, other from Bridge Biotherapeutics, personal fees and nonfinancial support from Canadian Respiratory Network, other from ProMedior, personal fees and nonfinancial support from Teva, personal fees from the France Foundation, personal fees and nonfinancial support from Dartmouth, other from Gala, and personal fees from Physicians Education Resource, outside the submitted work. Dr. Woodruff is a consultant for Astra Zeneca, Theravance, Glenmark pharmaceuticals, Sanofi, and Regeneron and has received funding from Genetech and the COPD Foundation. Dr. Hansel reports grants and personal fees from AstraZeneca, grants and personal fees from GSK, grants from Boehringer Ingelheim, grants from the NIH, and the COPD Foundation, and personal fees from Mylan, outside the submitted work. Dr. Hoffman is a founder and shareholder of VIDA Diagnostics, a company commercializing lung image analysis software developed, in part, at the University of Iowa. Dr. Peters reports grants from the NIH/NHLBI, during the conduct of the study; personal fees from Array Biopharma, personal fees from Integrity CE, personal fees from AstraZeneca, personal fees from Aerocrine, personal fees from Boehringer-Ingelheim, personal fees from Experts in Asthma, personal fees from Gilead, personal fees from GlaxoSmithKline, personal fees from Merck, personal fees from Novartis, personal fees from Ono Pharmaceuticals, personal fees from Pfizer, personal fees from PPD Development, personal fees from Quintiles, personal fees from Sunovion, personal fees from Saatchi & Saatichi, personal fees from Targacept, personal fees from TEVA, personal fees from Theron, personal fees from AstraZeneca, personal fees from Sanofi and Regeneron, and grants from the NIH/NHLBI, outside the submitted work. Dr. Ortega reports grants from the NIH, personal fees from CSL Behring, and personal fees from Regeneron and Sanofi for independent data and monitoring committee participation outside the submitted work.
References
-
- Woodruff PG,Barr RG,Bleecker E,et al. Clinical significance of symptoms in smokers with preserved pulmonary function. N Engl J Med. 2016;374(19):1811-1821. doi: https://doi.org/10.1056/NEJMoa1505971 - PMC - PubMed
-
- Purani H,Friedrichsen S,Allen AM. Sleep quality in cigarette smokers: associations with smoking-related outcomes and exercise. Addict Behav. 2019;90:71-76. doi: https://doi.org/10.1016/j.addbeh.2018.10.023 - PMC - PubMed
-
- Esen AD,Akpinar M. Relevance of obstructive sleep apnea and smoking: obstructive sleep apnea and smoking. Fam Pract. 2021;38(2):181-186. doi: https://doi.org/10.1093/fampra/cmaa112 - PubMed
-
- Omachi TA,Blanc PD,Claman DM,et al. Disturbed sleep among COPD patients is longitudinally associated with mortality and adverse COPD outcomes. Sleep Med. 2012;13(5):476-483. doi: https://doi.org/10.1016/j.sleep.2011.12.007 - PMC - PubMed
-
- Zeidler MR,Martin JL,Kleerup EC,et al. Sleep disruption as a predictor of quality of life among patients in the subpopulations and intermediate outcome measures in COPD study (SPIROMICS). Sleep. 2018;41(5):zsy044. doi: https://doi.org/10.1093/sleep/zsy044 - PMC - PubMed
Grants and funding
- HHSN268200900019C/HL/NHLBI NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- HHSN268200900015C/HL/NHLBI NIH HHS/United States
- HHSN268200900016C/HL/NHLBI NIH HHS/United States
- U01 HL137880/HL/NHLBI NIH HHS/United States
- HHSN268200900013C/HL/NHLBI NIH HHS/United States
- HHSN268200900014C/HL/NHLBI NIH HHS/United States
- U24 HL141762/HL/NHLBI NIH HHS/United States
- P30 ES010126/ES/NIEHS NIH HHS/United States
- HHSN268200900018C/HL/NHLBI NIH HHS/United States
- P30 DK054759/DK/NIDDK NIH HHS/United States
- HHSN268200900017C/HL/NHLBI NIH HHS/United States
- HHSN268200900020C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical