

Effect of implementing a heart failure admission care bundle on hospital readmission and mortality rates: interrupted time series study
- PMID: 37931935
- PMCID: PMC10804004
- DOI: 10.1136/bmjqs-2022-015511
Effect of implementing a heart failure admission care bundle on hospital readmission and mortality rates: interrupted time series study
Abstract
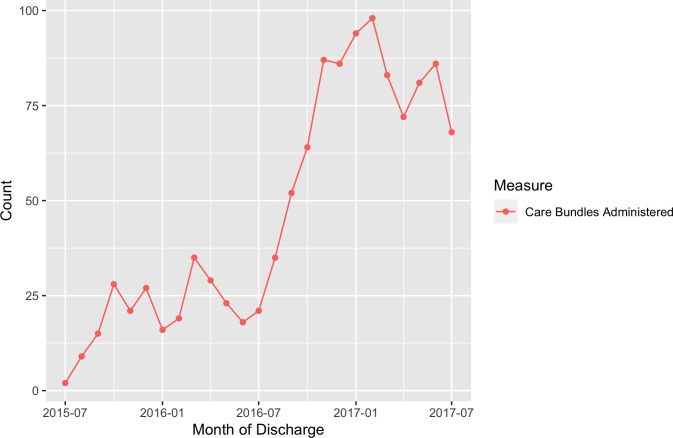
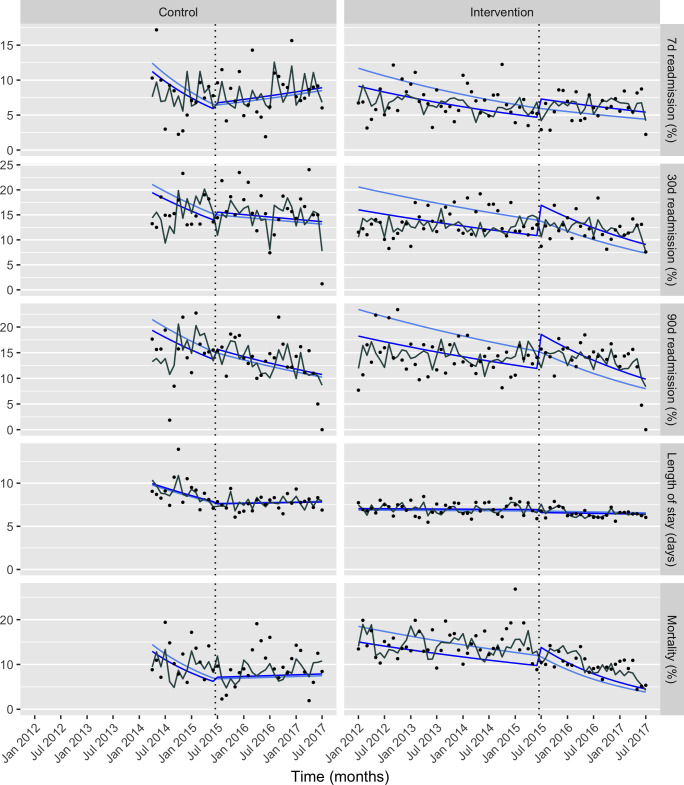
This study aimed to evaluate the impact of developing and implementing a care bundle intervention to improve care for patients with acute heart failure admitted to a large London hospital. The intervention comprised three elements, targeted within 24 hours of admission: N-terminal pro-B-type natriuretic peptide (NT-proBNP) test, transthoracic Doppler two-dimensional echocardiography and specialist review by cardiology team. The SHIFT-Evidence approach to quality improvement was used. During implementation, July 2015-July 2017, 1169 patients received the intervention. An interrupted time series design was used to evaluate impact on patient outcomes, including 15 618 admissions for 8951 patients. Mixed-effects multiple Poisson and log-linear regression models were fitted for count and continuous outcomes, respectively. Effect sizes are slope change ratios pre-intervention and post-intervention. The intervention was associated with reductions in emergency readmissions between 7 and 90 days (0.98, 95% CI 0.97 to 1.00), although not readmissions between 0 and 7 days post-discharge. Improvements were seen in in-hospital mortality (0.96, 95% CI 0.95 to 0.98), and there was no change in trend for hospital length of stay. Care process changes were also evaluated. Compliance with NT-proBNP testing was already high in 2014/2015 (162 of 163, 99.4%) and decreased slightly, with increased numbers audited, to 2016/2017 (1082 of 1101, 98.2%). Over this period, rates of echocardiography (84.7-98.9%) and specialist input (51.6-90.4%) improved. Care quality and outcomes can be improved for patients with acute heart failure using a care bundle approach. A systematic approach to quality improvement, and robust evaluation design, can be beneficial in supporting successful improvement and learning.
Keywords: Evaluation methodology; Healthcare quality improvement; Implementation science.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: MRC has been employed by AstraZeneca since 1 August 2022.
Figures
References
-
- NHS England » 2013/14 NHS standard contract. Available: https://www.england.nhs.uk/nhs-standard-contract/previous-nhs-standard-c... [Accessed 2 Aug 2023].
-
- National Institute for Cardiovascular Outcomes Research (NICOR), Institute of Cardiovascular Science, University College London . British society for heart failure 2; 2015. Available: https://www.nicor.org.uk/wp-content/uploads/2019/02/annual_report_2014_1... [Accessed 19 Oct 2023].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials