

Diabetes Mellitus, Energy Metabolism, and COVID-19
- PMID: 37934800
- PMCID: PMC10911957
- DOI: 10.1210/endrev/bnad032
Diabetes Mellitus, Energy Metabolism, and COVID-19
Abstract
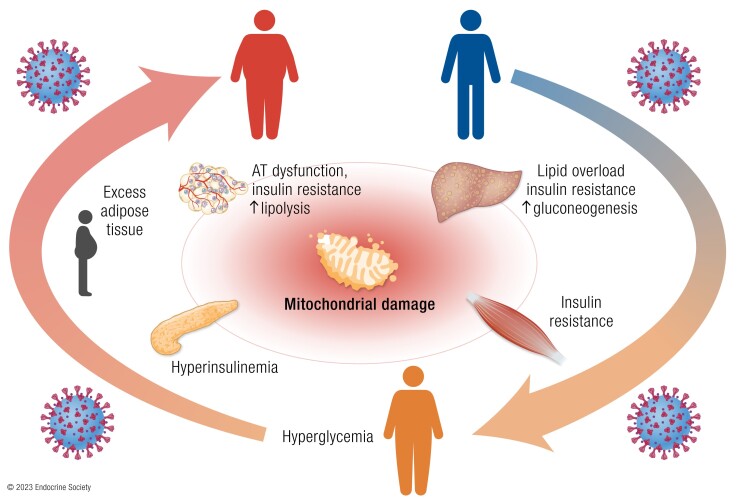
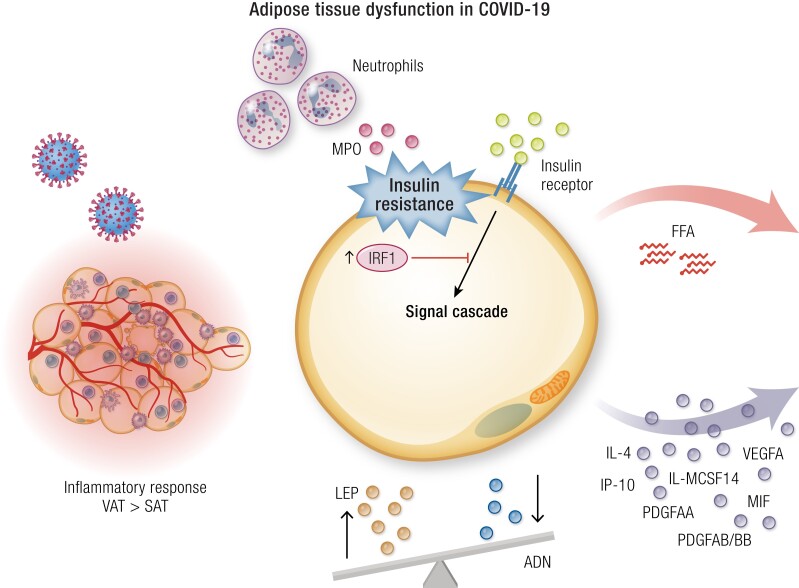
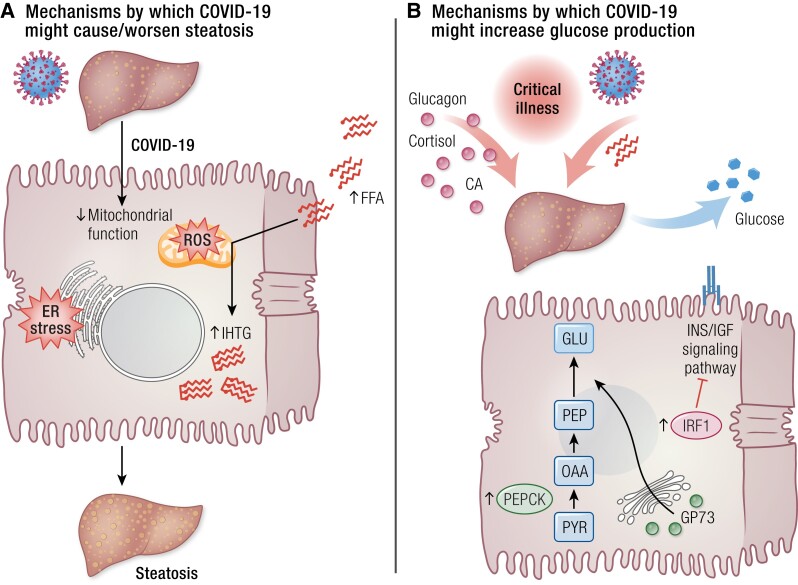
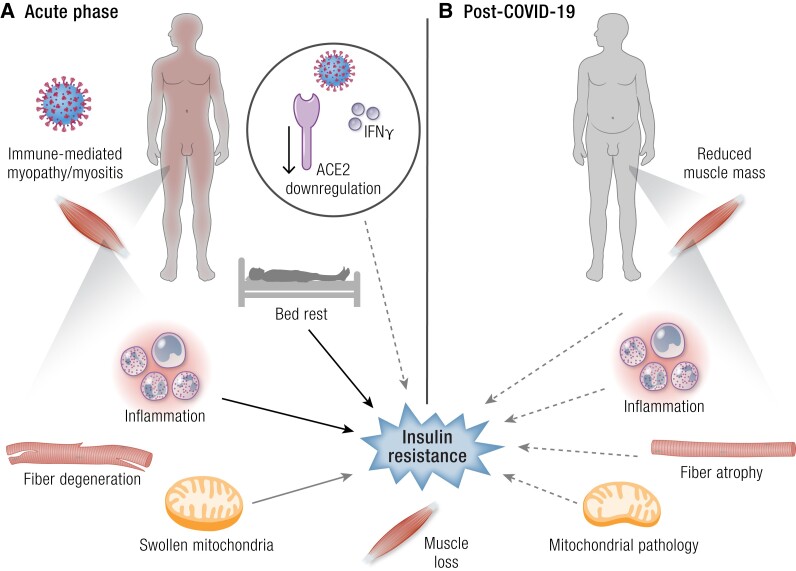
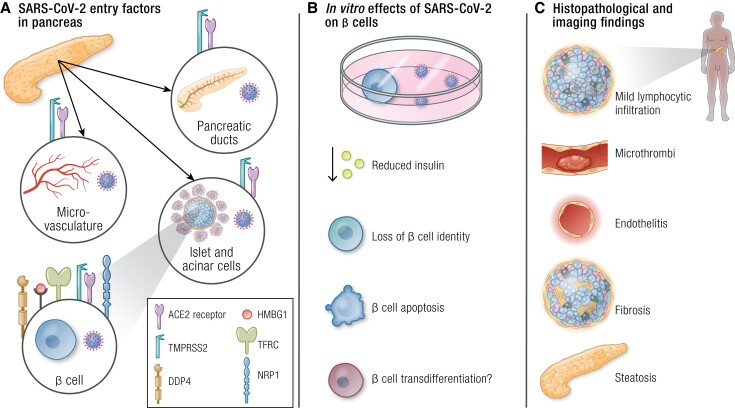
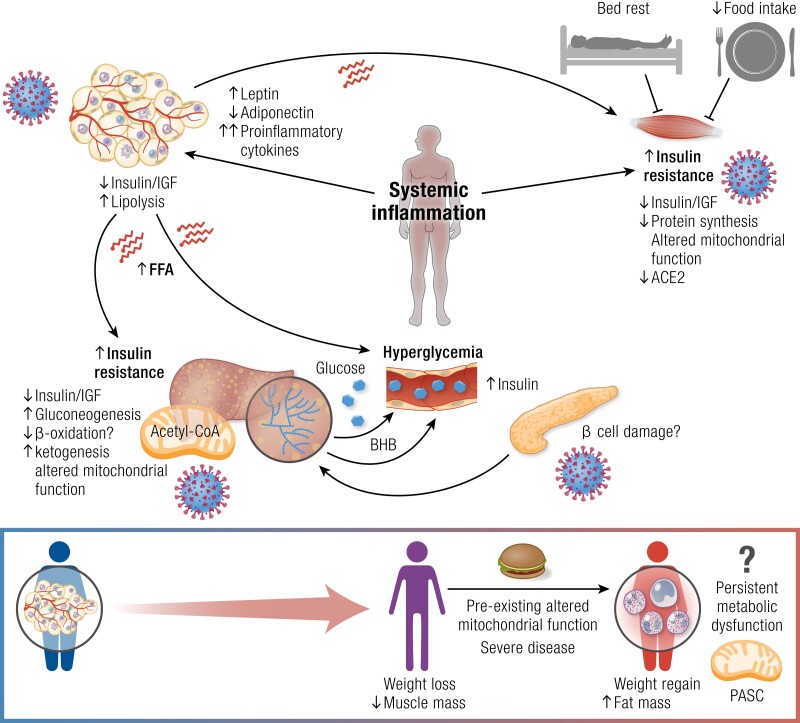
Obesity, diabetes mellitus (mostly type 2), and COVID-19 show mutual interactions because they are not only risk factors for both acute and chronic COVID-19 manifestations, but also because COVID-19 alters energy metabolism. Such metabolic alterations can lead to dysglycemia and long-lasting effects. Thus, the COVID-19 pandemic has the potential for a further rise of the diabetes pandemic. This review outlines how preexisting metabolic alterations spanning from excess visceral adipose tissue to hyperglycemia and overt diabetes may exacerbate COVID-19 severity. We also summarize the different effects of SARS-CoV-2 infection on the key organs and tissues orchestrating energy metabolism, including adipose tissue, liver, skeletal muscle, and pancreas. Last, we provide an integrative view of the metabolic derangements that occur during COVID-19. Altogether, this review allows for better understanding of the metabolic derangements occurring when a fire starts from a small flame, and thereby help reducing the impact of the COVID-19 pandemic.
Keywords: SARS-CoV-2; adipose tissue; diabetes; liver; pancreas; skeletal muscle.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Similar articles
-
Post-COVID syndrome, inflammation, and diabetes.J Diabetes Complications. 2022 Nov;36(11):108336. doi: 10.1016/j.jdiacomp.2022.108336. Epub 2022 Oct 6. J Diabetes Complications. 2022. PMID: 36228563 Free PMC article. Review.
-
SARS-CoV-2 perturbs the renin-angiotensin system and energy metabolism.Am J Physiol Endocrinol Metab. 2020 Jul 1;319(1):E43-E47. doi: 10.1152/ajpendo.00219.2020. Epub 2020 May 29. Am J Physiol Endocrinol Metab. 2020. PMID: 32469255 Free PMC article.
-
COVID-19 and diabetes mellitus: a review of the incidence, pathophysiology and management of diabetes during the pandemic.Expert Rev Endocrinol Metab. 2023 Mar;18(2):167-179. doi: 10.1080/17446651.2023.2176300. Epub 2023 Feb 16. Expert Rev Endocrinol Metab. 2023. PMID: 36797835 Review.
-
SARS-CoV-2 infection impairs the insulin/IGF signaling pathway in the lung, liver, adipose tissue, and pancreatic cells via IRF1.Metabolism. 2022 Aug;133:155236. doi: 10.1016/j.metabol.2022.155236. Epub 2022 Jun 8. Metabolism. 2022. PMID: 35688210 Free PMC article.
-
Unwinding Link between Coronavirus and Diabetes Patient.Endocr Metab Immune Disord Drug Targets. 2022;22(11):1091-1110. doi: 10.2174/1871530322666220329150238. Endocr Metab Immune Disord Drug Targets. 2022. PMID: 35352656
Cited by
-
Sex differences in patients with COVID-19 after bariatric surgery: a multicenter cross-sectional study.Front Public Health. 2024 Jan 15;11:1293318. doi: 10.3389/fpubh.2023.1293318. eCollection 2023. Front Public Health. 2024. PMID: 38288424 Free PMC article.
-
Critical COVID-19, Victivallaceae abundance, and celiac disease: A mediation Mendelian randomization study.PLoS One. 2024 May 3;19(5):e0301998. doi: 10.1371/journal.pone.0301998. eCollection 2024. PLoS One. 2024. PMID: 38701071 Free PMC article.
-
Host factors of SARS-CoV-2 in infection, pathogenesis, and long-term effects.Front Cell Infect Microbiol. 2024 May 22;14:1407261. doi: 10.3389/fcimb.2024.1407261. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38846354 Free PMC article. Review.
-
Alterations of hepatic lipid content following COVID-19 in persons with type 2 diabetes.BMJ Open Diabetes Res Care. 2025 Feb 18;13(1):e004727. doi: 10.1136/bmjdrc-2024-004727. BMJ Open Diabetes Res Care. 2025. PMID: 39965871 Free PMC article.
-
Energy metabolism in health and diseases.Signal Transduct Target Ther. 2025 Feb 18;10(1):69. doi: 10.1038/s41392-025-02141-x. Signal Transduct Target Ther. 2025. PMID: 39966374 Free PMC article. Review.
References
-
- World Health Organization . WHO Coronavirus Disease (COVID-19) Dashboard. Available athttps://covid19.who.int/. 2020.
