

High contrast cartilaginous endplate imaging in spine using three dimensional dual-inversion recovery prepared ultrashort echo time (3D DIR-UTE) sequence
- PMID: 37935923
- PMCID: PMC10973042
- DOI: 10.1007/s00256-023-04503-4
High contrast cartilaginous endplate imaging in spine using three dimensional dual-inversion recovery prepared ultrashort echo time (3D DIR-UTE) sequence
Abstract
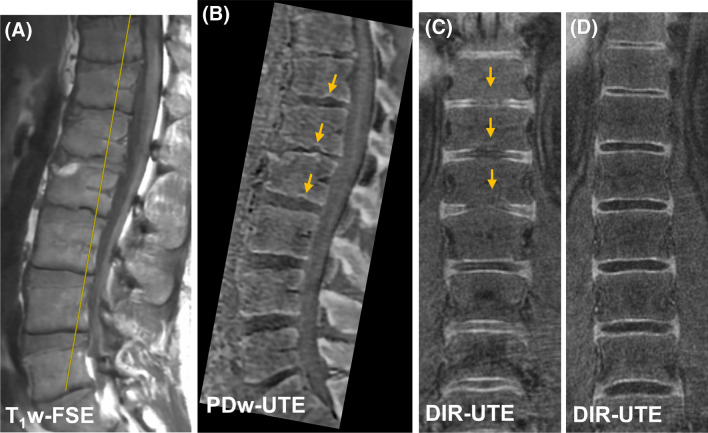
Purpose: To investigate the feasibility and application of a novel imaging technique, a three-dimensional dual adiabatic inversion recovery prepared ultrashort echo time (3D DIR-UTE) sequence, for high contrast assessment of cartilaginous endplate (CEP) imaging with head-to-head comparisons between other UTE imaging techniques.
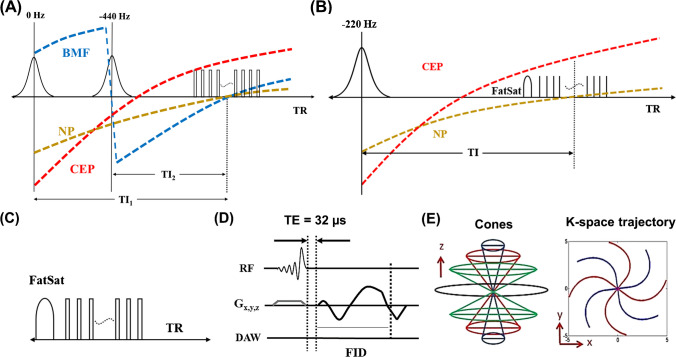
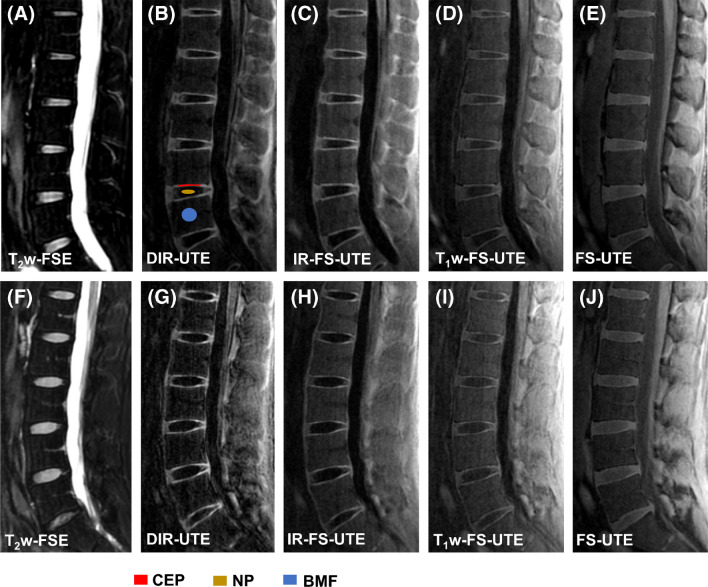
Method: The DIR-UTE sequence employs two narrow-band adiabatic full passage (AFP) pulses to suppress signals from long T2 water (e.g., nucleus pulposus (NP)) and bone marrow fat (BMF) independently, followed by multispoke UTE acquisition to detect signals from the CEP with short T2 relaxation times. The DIR-UTE sequence, in addition to three other UTE sequences namely, an IR-prepared and fat-saturated UTE (IR-FS-UTE), a T1-weighted and fat-saturated UTE sequence (T1w-FS-UTE), and a fat-saturated UTE (FS-UTE) was used for MR imaging on a 3 T scanner to image six asymptomatic volunteers, six patients with low back pain, as well as a human cadaveric specimen. The contrast-to-noise ratio of the CEP relative to the adjacent structures-specifically the NP and BMF-was then compared from the acquired images across the different UTE sequences.
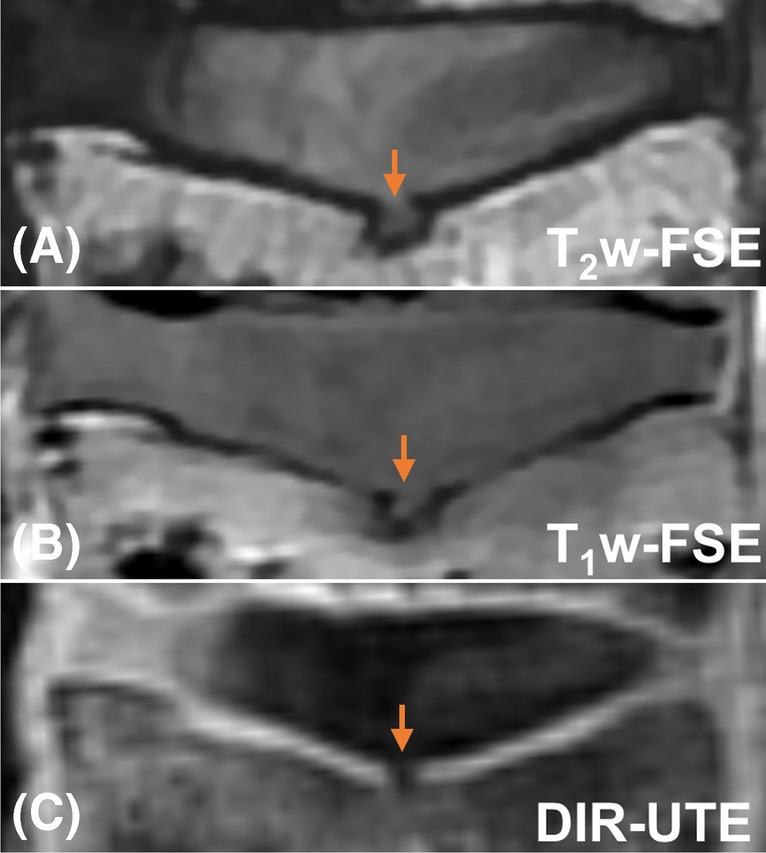
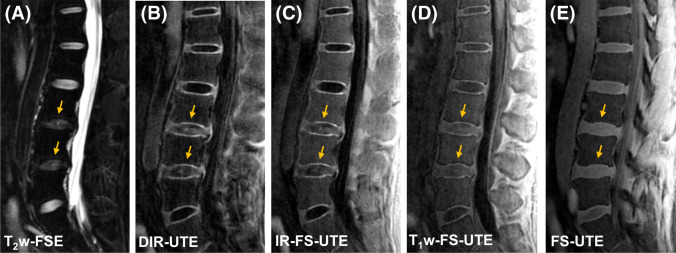
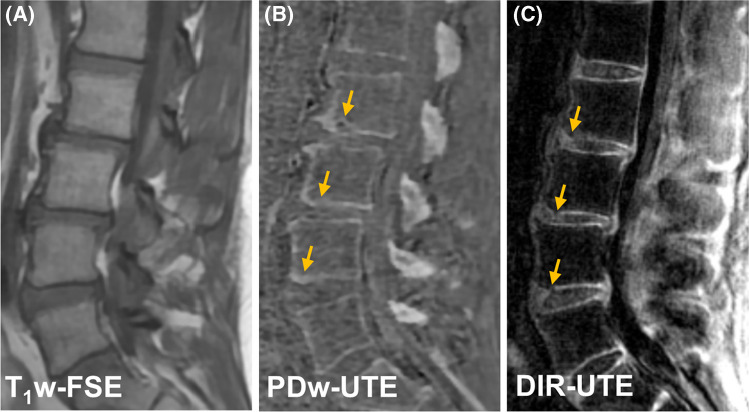
Results: For asymptomatic volunteers, the DIR-UTE sequence showed significantly higher contrast-to-noise ratio values between the CEP and BMF (CNRCEP-BMF) (19.9 ± 3.0) and between the CEP and NP (CNRCEP-NP) (23.1 ± 1.7) compared to IR-FS-UTE (CNRCEP-BMF: 17.3 ± 1.2 and CNRCEP-NP: 19.1 ± 1.8), T1w-FS-UTE (CNRCEP-BMF: 9.0 ± 2.7 and CNRCEP-NP: 10.4 ± 3.5), and FS-UTE (CNRCEP-BMF: 7.7 ± 2.2 and CNRCEP-NP: 5.8 ± 2.4) for asymptomatic volunteers (all P-values < 0.001). For the spine sample and patients with low back pain, the DIR-UTE technique detected abnormalities such as irregularities and focal defects in the CEP regions.
Conclusion: The 3D DIR-UTE sequence is able to provide high-contrast volumetric CEP imaging for human spines on a clinical 3 T scanner.
Keywords: Cartilaginous endplate; Dual adiabatic inversion recovery; High contrast; Low back pain; UTE.
© 2023. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Evaluation of spine disorders using high contrast imaging of the cartilaginous endplate.Front Physiol. 2024 May 27;15:1394189. doi: 10.3389/fphys.2024.1394189. eCollection 2024. Front Physiol. 2024. PMID: 38860112 Free PMC article.
-
Qualitative and Quantitative MR Imaging of the Cartilaginous Endplate: A Review.J Magn Reson Imaging. 2025 Apr;61(4):1552-1571. doi: 10.1002/jmri.29562. Epub 2024 Aug 20. J Magn Reson Imaging. 2025. PMID: 39165086 Review.
-
High contrast cartilaginous endplate imaging using a 3D adiabatic inversion-recovery-prepared fat-saturated ultrashort echo time (3D IR-FS-UTE) sequence.NMR Biomed. 2021 Oct;34(10):e4579. doi: 10.1002/nbm.4579. Epub 2021 Jul 5. NMR Biomed. 2021. PMID: 34219287 Free PMC article.
-
High-contrast osteochondral junction imaging using a 3D dual adiabatic inversion recovery-prepared ultrashort echo time cones sequence.NMR Biomed. 2021 Aug;34(8):e4559. doi: 10.1002/nbm.4559. Epub 2021 May 22. NMR Biomed. 2021. PMID: 34021649 Free PMC article.
-
An Update in Qualitative Imaging of Bone Using Ultrashort Echo Time Magnetic Resonance.Front Endocrinol (Lausanne). 2020 Sep 29;11:555756. doi: 10.3389/fendo.2020.555756. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 33117275 Free PMC article. Review.
Cited by
-
Evaluation of spine disorders using high contrast imaging of the cartilaginous endplate.Front Physiol. 2024 May 27;15:1394189. doi: 10.3389/fphys.2024.1394189. eCollection 2024. Front Physiol. 2024. PMID: 38860112 Free PMC article.
-
Qualitative and Quantitative MR Imaging of the Cartilaginous Endplate: A Review.J Magn Reson Imaging. 2025 Apr;61(4):1552-1571. doi: 10.1002/jmri.29562. Epub 2024 Aug 20. J Magn Reson Imaging. 2025. PMID: 39165086 Review.
-
Cartilaginous endplate coverage of developmental Schmorl's node and the relevance of this in Schmorl's node etiology-based classification.Quant Imaging Med Surg. 2024 Jun 1;14(6):4288-4303. doi: 10.21037/qims-24-335. Epub 2024 May 9. Quant Imaging Med Surg. 2024. PMID: 38846309 Free PMC article. No abstract available.
-
Ultrashort-Echo-Time MRI of the Disco-Vertebral Junction: Modulation of Image Contrast via Echo Subtraction and Echo Times.Sensors (Basel). 2024 Sep 9;24(17):5842. doi: 10.3390/s24175842. Sensors (Basel). 2024. PMID: 39275753 Free PMC article.
References
MeSH terms
Grants and funding
- R01 AR068987/AR/NIAMS NIH HHS/United States
- K01AR080257/GF/NIH HHS/United States
- R21 AR075851/AR/NIAMS NIH HHS/United States
- T32 AR007581/AR/NIAMS NIH HHS/United States
- R01AR075825/GF/NIH HHS/United States
- F32 AG082458/AG/NIA NIH HHS/United States
- R01 AR062581/AR/NIAMS NIH HHS/United States
- R01AR068987/GF/NIH HHS/United States
- I01 CX001388/CX/CSRD VA/United States
- R01AR079484/GF/NIH HHS/United States
- I01 RX002604/RX/RRD VA/United States
- R01 AR075825/AR/NIAMS NIH HHS/United States
- R21AR07581/GF/NIH HHS/United States
- R01 AR079484/AR/NIAMS NIH HHS/United States
- F32AG082458/GF/NIH HHS/United States
- K01 AR080257/AR/NIAMS NIH HHS/United States
- R01AR062581/GF/NIH HHS/United States
LinkOut - more resources
Full Text Sources
Miscellaneous
