

Systematic review and meta-analysis of the effects of menopause hormone therapy on risk of Alzheimer's disease and dementia
- PMID: 37937120
- PMCID: PMC10625913
- DOI: 10.3389/fnagi.2023.1260427
Systematic review and meta-analysis of the effects of menopause hormone therapy on risk of Alzheimer's disease and dementia
Abstract
Introduction: Despite a large preclinical literature demonstrating neuroprotective effects of estrogen, use of menopausal hormone therapy (HT) for Alzheimer's disease (AD) risk reduction has been controversial. Herein, we conducted a systematic review and meta-analysis of HT effects on AD and dementia risk.
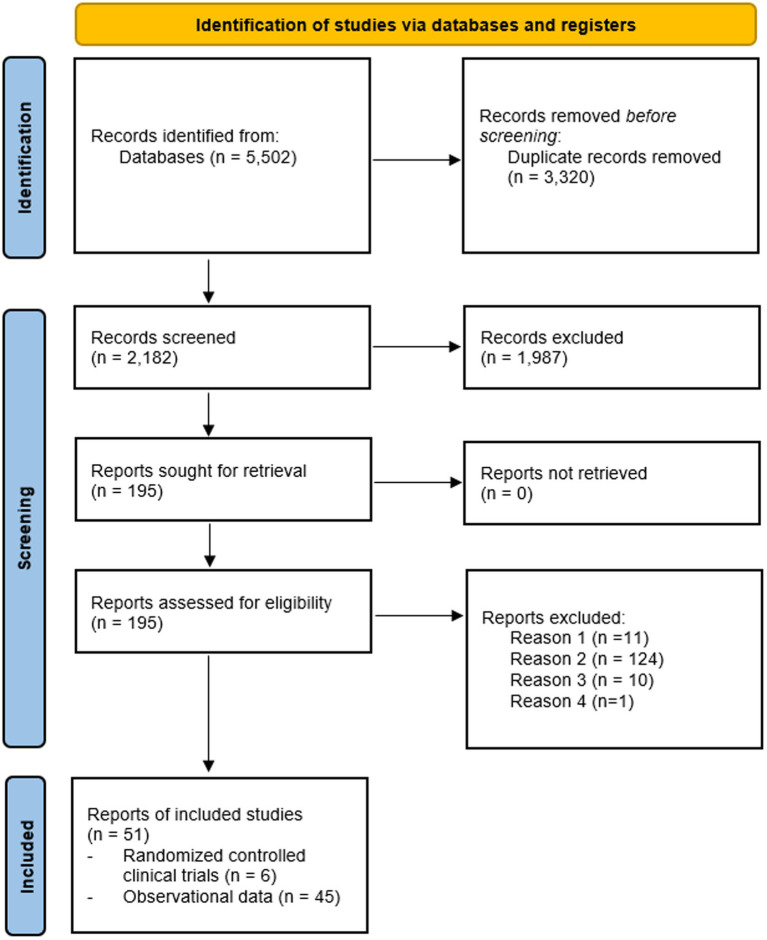
Methods: Our systematic search yielded 6 RCT reports (21,065 treated and 20,997 placebo participants) and 45 observational reports (768,866 patient cases and 5.5 million controls). We used fixed and random effect meta-analysis to derive pooled relative risk (RR) and 95% confidence intervals (C.I.) from these studies.
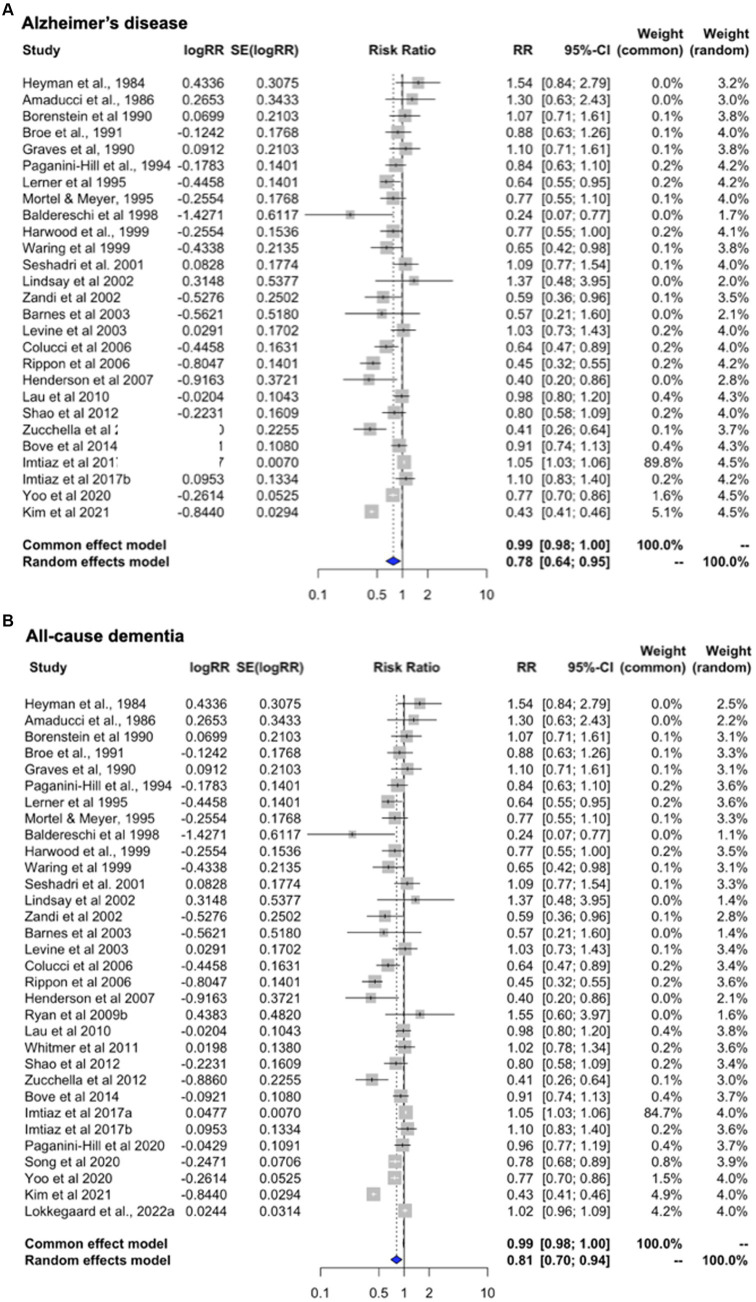
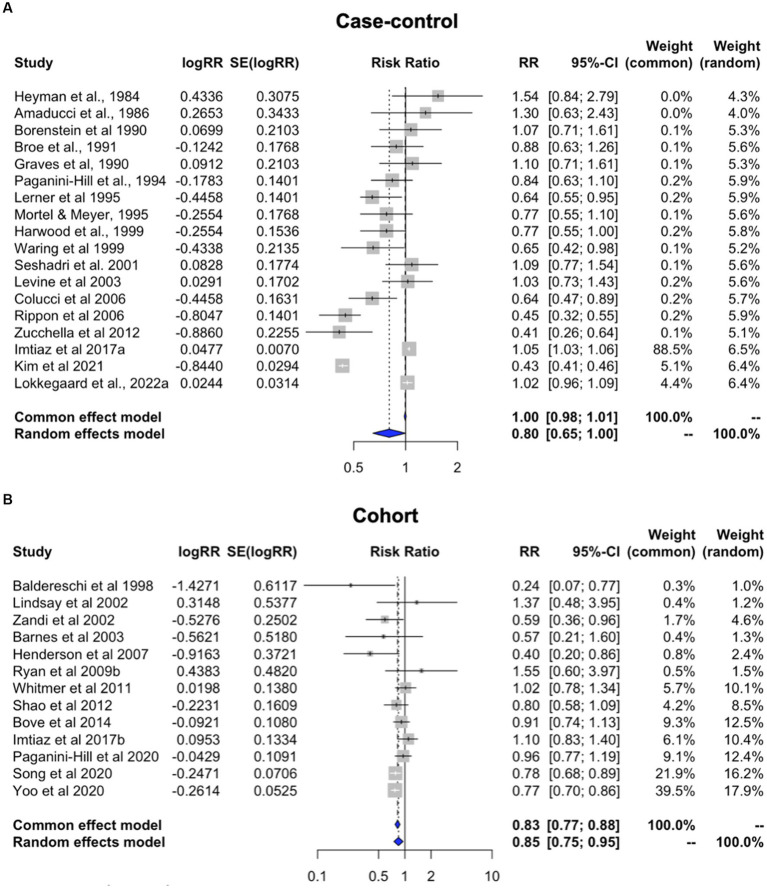
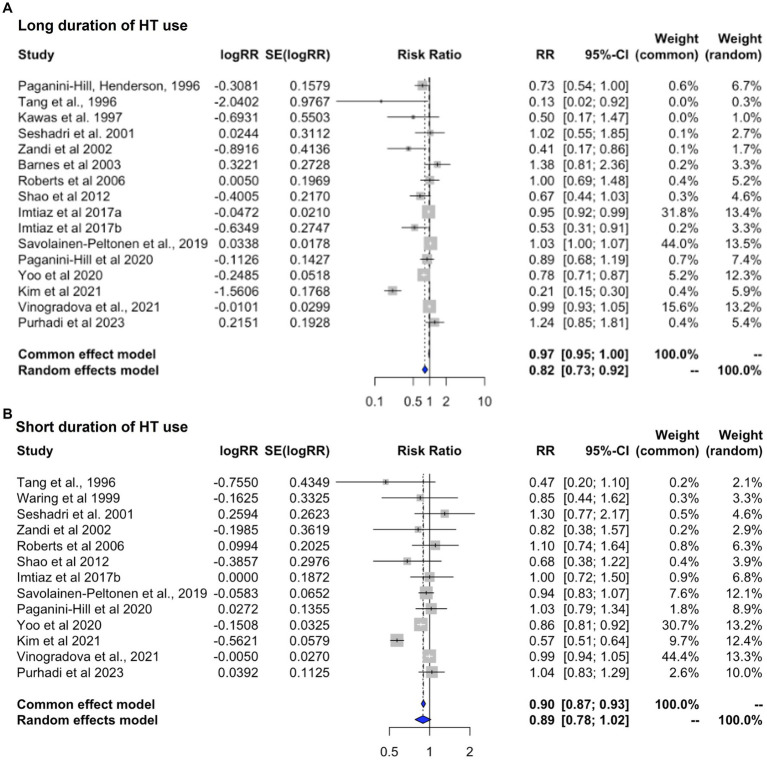
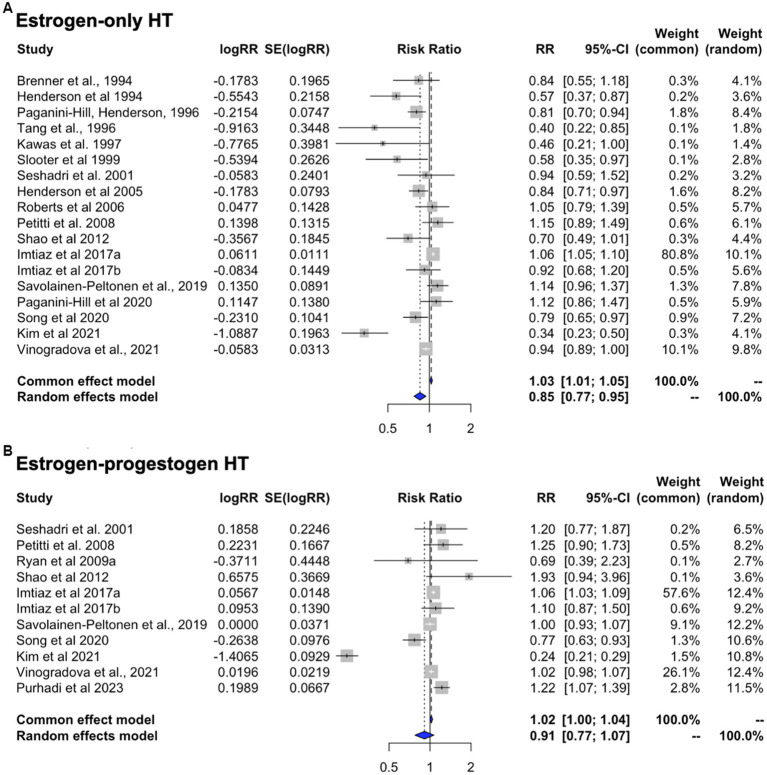
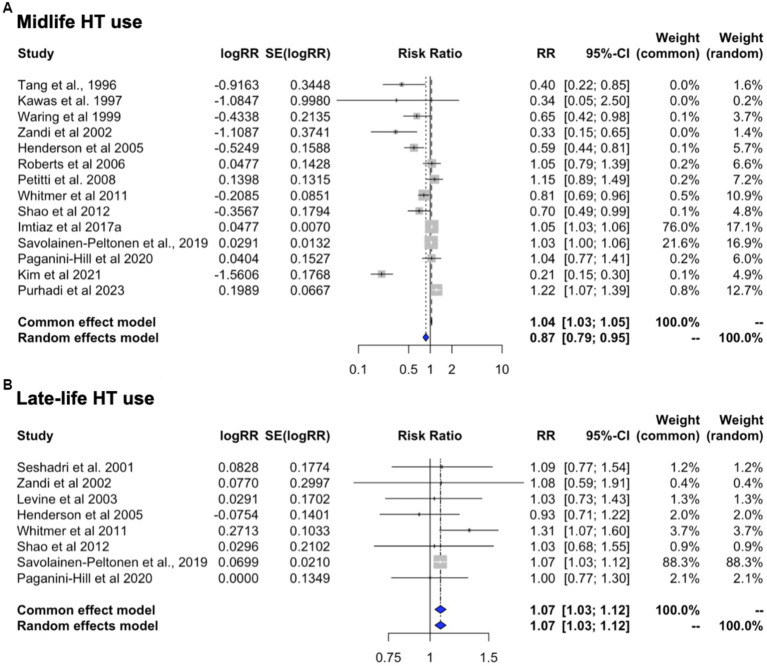
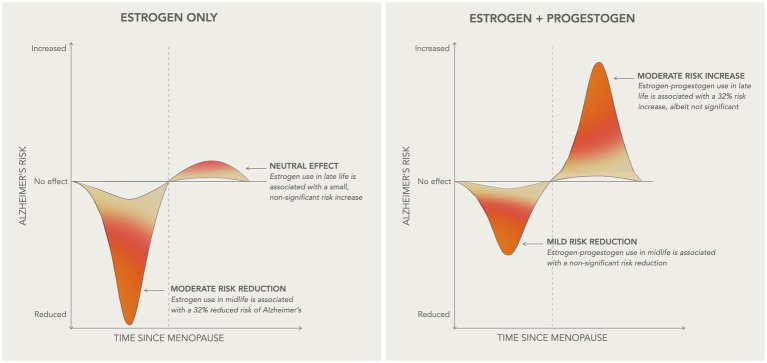
Results: Randomized controlled trials conducted in postmenopausal women ages 65 and older show an increased risk of dementia with HT use compared with placebo [RR = 1.38, 95% C.I. 1.16-1.64, p < 0.001], driven by estrogen-plus-progestogen therapy (EPT) [RR = 1.64, 95% C.I. 1.20-2.25, p = 0.002] and no significant effects of estrogen-only therapy (ET) [RR = 1.19, 95% C.I. 0.92-1.54, p = 0.18]. Conversely, observational studies indicate a reduced risk of AD [RR = 0.78, 95% C.I. 0.64-0.95, p = 0.013] and all-cause dementia [RR = .81, 95% C.I. 0.70-0.94, p = 0.007] with HT use, with protective effects noted with ET [RR = 0.86, 95% C.I. 0.77-0.95, p = 0.002] but not with EPT [RR = 0.910, 95% C.I. 0.775-1.069, p = 0.251]. Stratified analysis of pooled estimates indicates a 32% reduced risk of dementia with midlife ET [RR = 0.685, 95% C.I. 0.513-0.915, p = 0.010] and non-significant reductions with midlife EPT [RR = 0.775, 95% C.I. 0.474-1.266, p = 0.309]. Late-life HT use was associated with increased risk, albeit not significant [EPT: RR = 1.323, 95% C.I. 0.979-1.789, p = 0.069; ET: RR = 1.066, 95% C.I. 0.996-1.140, p = 0.066].
Discussion: These findings support renewed research interest in evaluating midlife estrogen therapy for AD risk reduction.
Keywords: Alzheimer’s disease; dementia; menopause hormonal therapy; meta-analysis; systematic review.
Copyright © 2023 Nerattini, Jett, Andy, Carlton, Zarate, Boneu, Battista, Pahlajani, Loeb-Zeitlin, Havryulik, Williams, Christos, Fink, Brinton and Mosconi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources