

Routine Metagenomics Service for ICU Patients with Respiratory Infection
- PMID: 37938162
- PMCID: PMC10806431
- DOI: 10.1164/rccm.202305-0901OC
Routine Metagenomics Service for ICU Patients with Respiratory Infection
Abstract
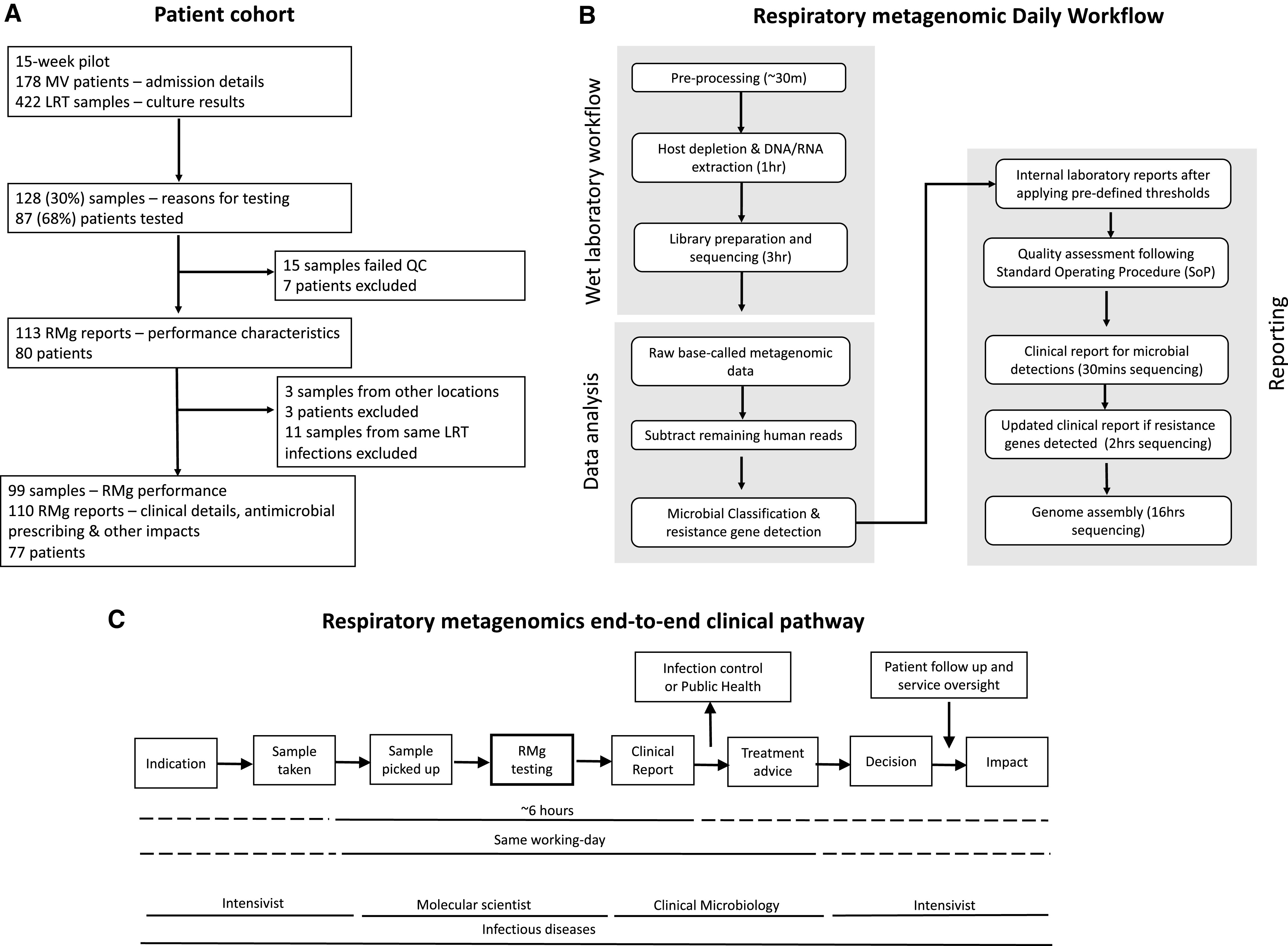
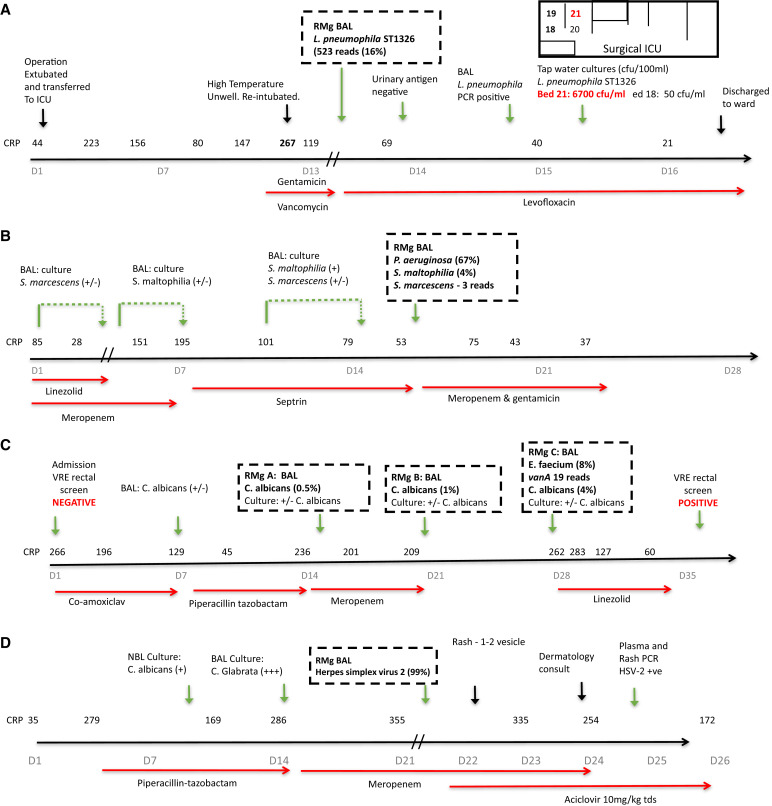
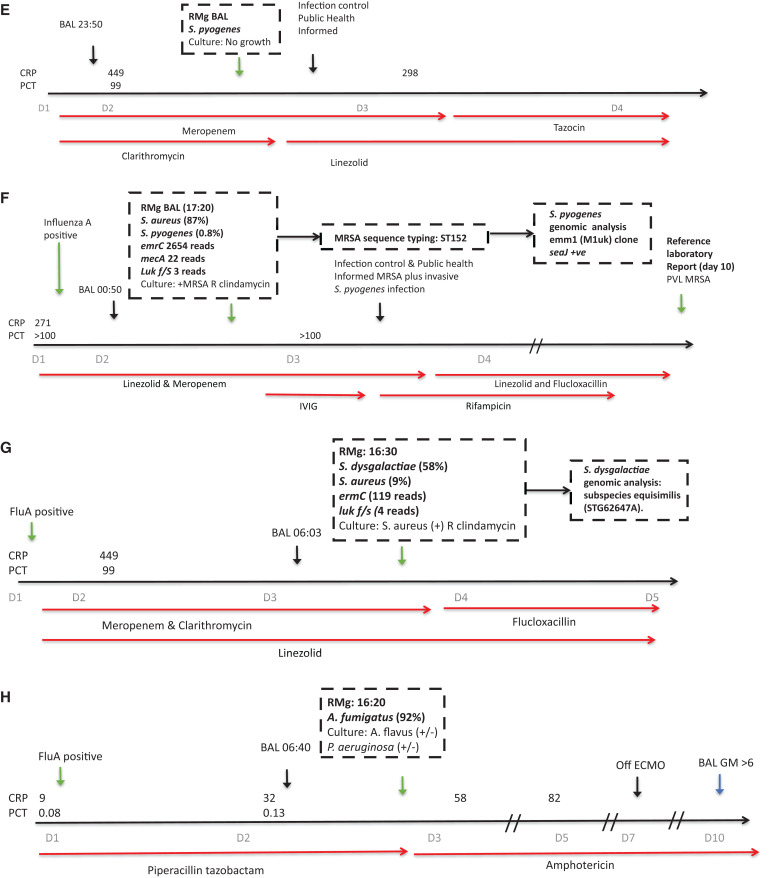
Rationale: Respiratory metagenomics (RMg) needs evaluation in a pilot service setting to determine utility and inform implementation into routine clinical practice. Objectives: Feasibility, performance, and clinical impacts on antimicrobial prescribing and infection control were recorded during a pilot RMg service. Methods: RMg was performed on 128 samples from 87 patients with suspected lower respiratory tract infection (LRTI) on two general and one specialist respiratory ICUs at Guy's and St Thomas' NHS Foundation Trust, London. Measurements and Main Results: During the first 15 weeks, RMg provided same-day results for 110 samples (86%), with a median turnaround time of 6.7 hours (interquartile range = 6.1-7.5 h). RMg was 93% sensitive and 81% specific for clinically relevant pathogens compared with routine testing. Forty-eight percent of RMg results informed antimicrobial prescribing changes (22% escalation; 26% deescalation) with escalation based on speciation in 20 out of 24 cases and detection of acquired-resistance genes in 4 out of 24 cases. Fastidious or unexpected organisms were reported in 21 samples, including anaerobes (n = 12), Mycobacterium tuberculosis, Tropheryma whipplei, cytomegalovirus, and Legionella pneumophila ST1326, which was subsequently isolated from the bedside water outlet. Application to consecutive severe community-acquired LRTI cases identified Staphylococcus aureus (two with SCCmec and three with luk F/S virulence determinants), Streptococcus pyogenes (emm1-M1uk clone), S. dysgalactiae subspecies equisimilis (STG62647A), and Aspergillus fumigatus with multiple treatments and public health impacts. Conclusions: This pilot study illustrates the potential of RMg testing to provide benefits for antimicrobial treatment, infection control, and public health when provided in a real-world critical care setting. Multicenter studies are now required to inform future translation into routine service.
Figures
Comment in
-
Respiratory Metagenomics: Ready for Prime Time?Am J Respir Crit Care Med. 2024 Jan 15;209(2):124-126. doi: 10.1164/rccm.202311-2039ED. Am J Respir Crit Care Med. 2024. PMID: 38029295 Free PMC article. No abstract available.
References
-
- Cookson WOCM, Cox MJ, Moffatt MF. New opportunities for managing acute and chronic lung infections. Nat Rev Microbiol . 2018;16:111–120. - PubMed
-
- Charalampous T, Alcolea-Medina A, Snell LB, Williams TGS, Batra R, Alder C, et al. Evaluating the potential for respiratory metagenomics to improve treatment of secondary infection and detection of nosocomial transmission on expanded COVID-19 intensive care units. Genome Med . 2021;13:182. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
