

Inflammation in the tumor-adjacent lung as a predictor of clinical outcome in lung adenocarcinoma
- PMID: 37938580
- PMCID: PMC10632519
- DOI: 10.1038/s41467-023-42327-x
Inflammation in the tumor-adjacent lung as a predictor of clinical outcome in lung adenocarcinoma
Abstract
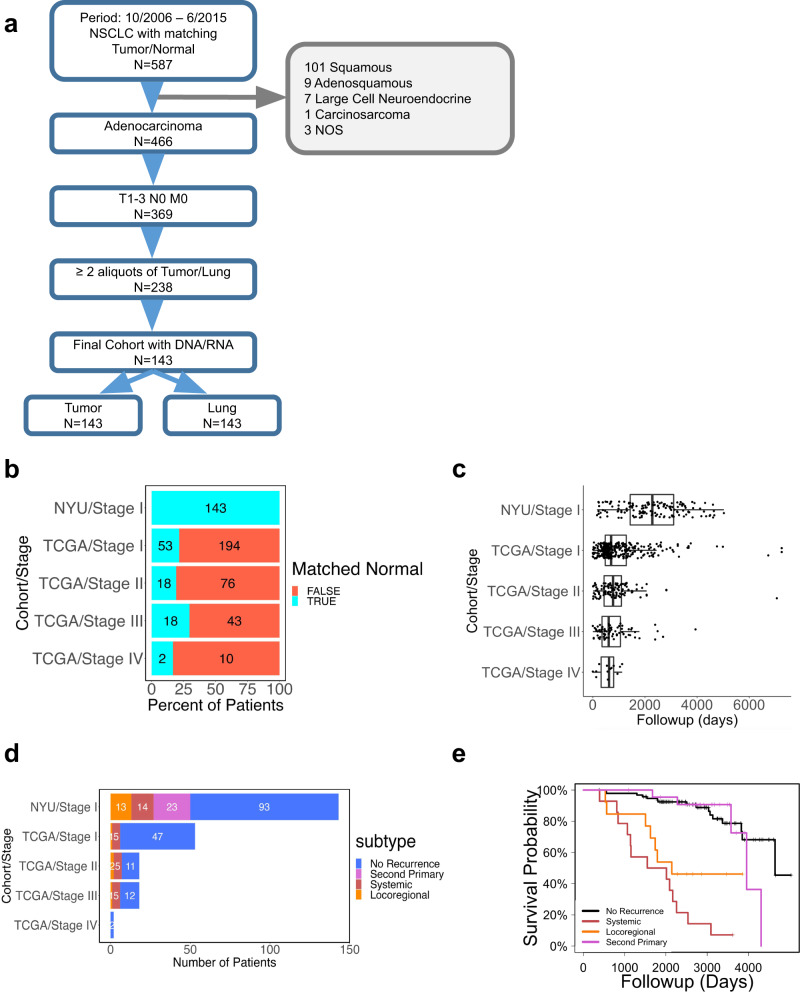
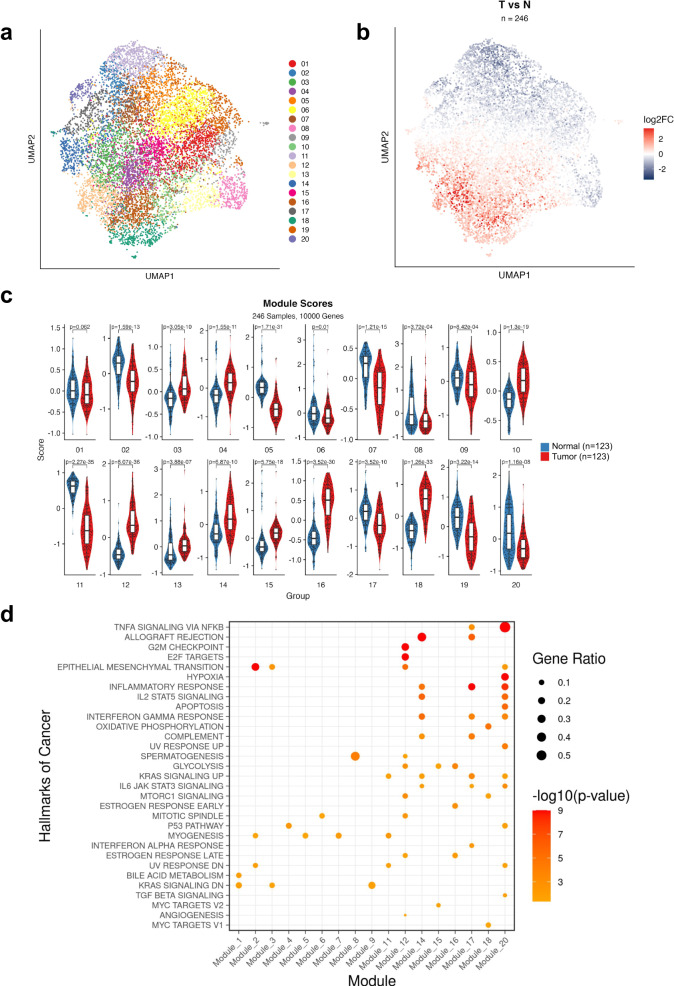
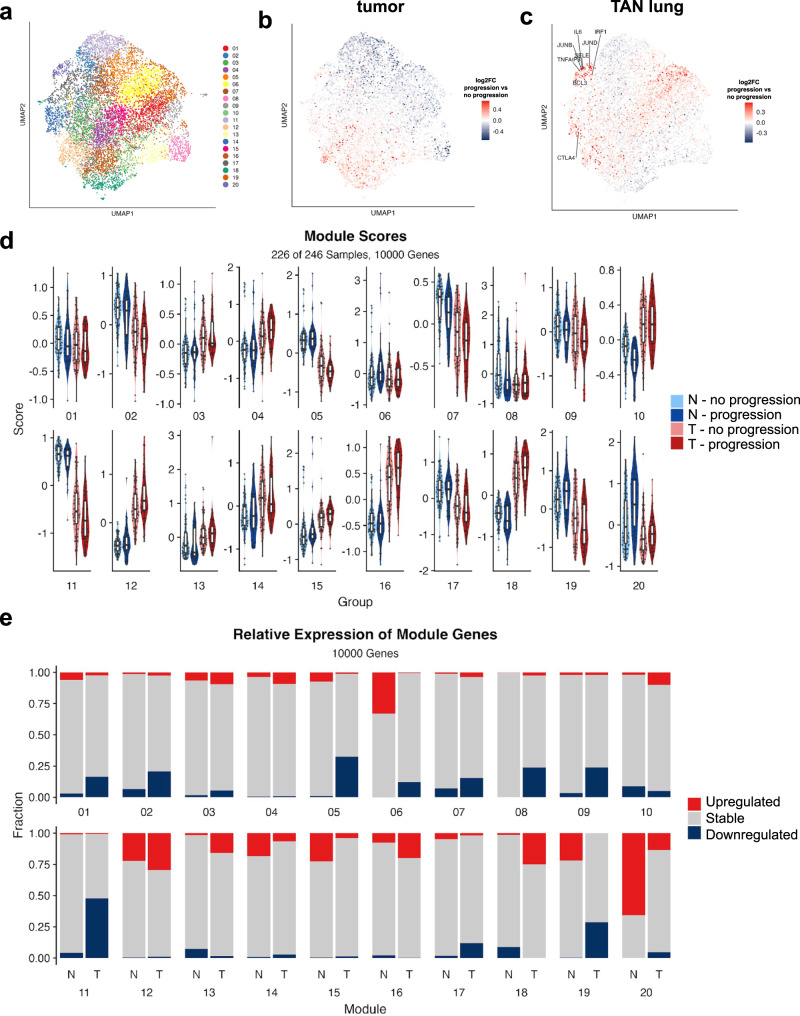
Approximately 30% of early-stage lung adenocarcinoma patients present with disease progression after successful surgical resection. Despite efforts of mapping the genetic landscape, there has been limited success in discovering predictive biomarkers of disease outcomes. Here we performed a systematic multi-omic assessment of 143 tumors and matched tumor-adjacent, histologically-normal lung tissue with long-term patient follow-up. Through histologic, mutational, and transcriptomic profiling of tumor and adjacent-normal tissue, we identified an inflammatory gene signature in tumor-adjacent tissue as the strongest clinical predictor of disease progression. Single-cell transcriptomic analysis demonstrated the progression-associated inflammatory signature was expressed in both immune and non-immune cells, and cell type-specific profiling in monocytes further improved outcome predictions. Additional analyses of tumor-adjacent transcriptomic data from The Cancer Genome Atlas validated the association of the inflammatory signature with worse outcomes across cancers. Collectively, our study suggests that molecular profiling of tumor-adjacent tissue can identify patients at high risk for disease progression.
© 2023. Springer Nature Limited.
Conflict of interest statement
A.T. is a scientific advisor to Intelligencia AI. The remaining authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
