

Prognostic association supports indexing size measures in echocardiography by body surface area
- PMID: 37938592
- PMCID: PMC10632399
- DOI: 10.1038/s41598-023-46183-z
Prognostic association supports indexing size measures in echocardiography by body surface area
Abstract
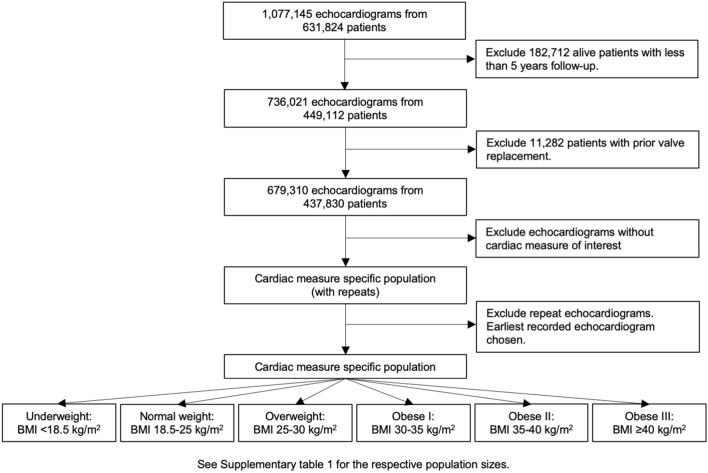
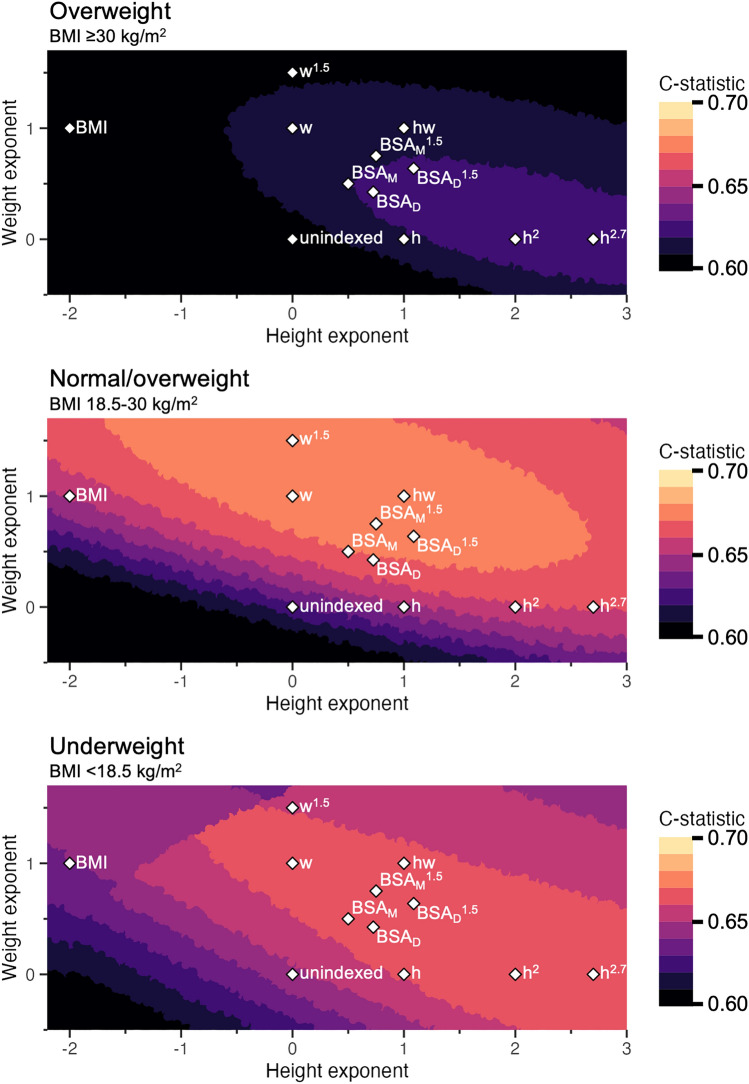
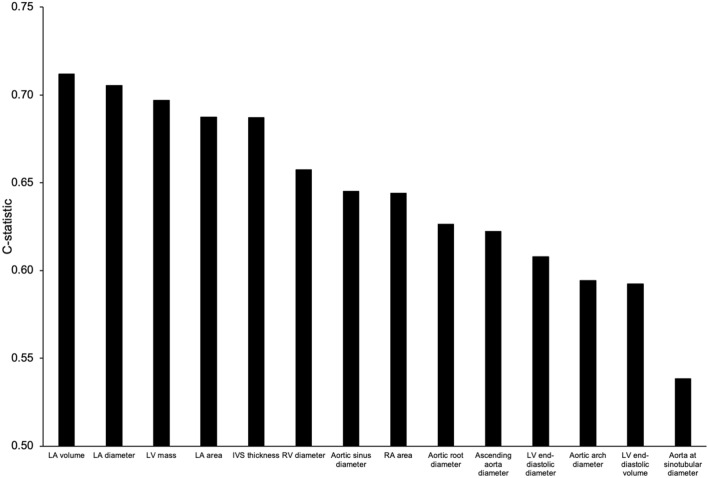
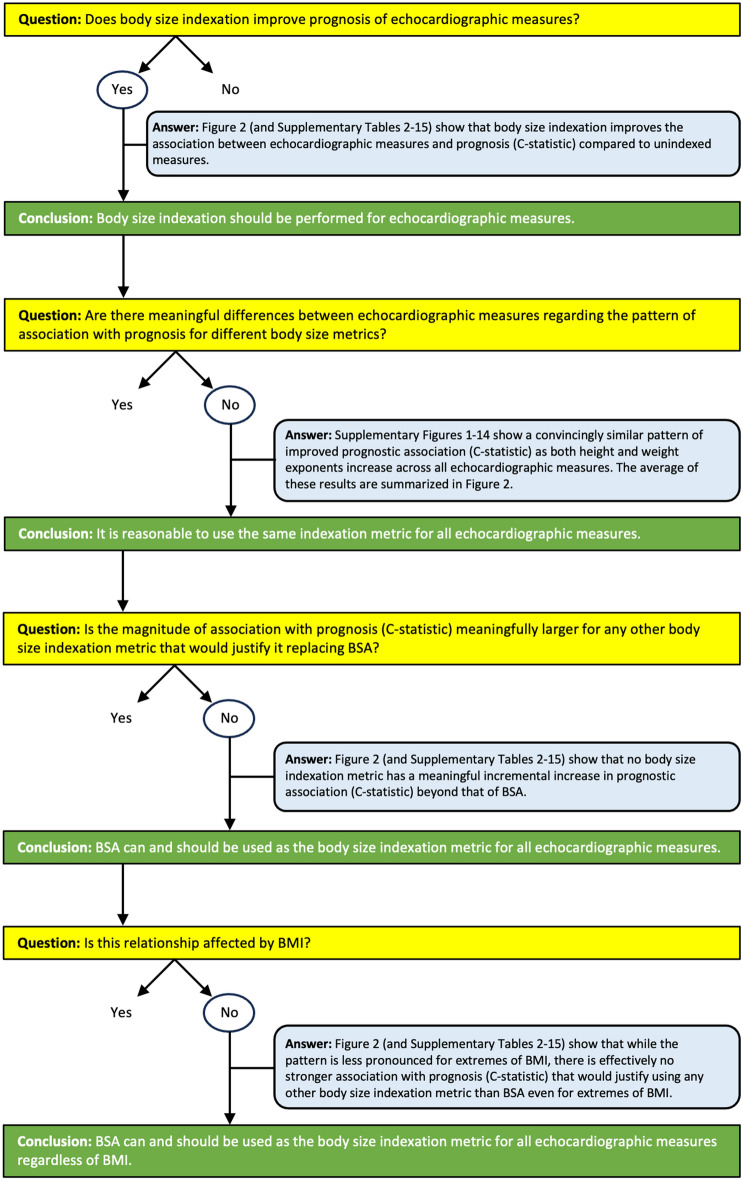
Body surface area (BSA) is the most commonly used metric for body size indexation of echocardiographic measures, but its use in patients who are underweight or obese is questioned (body mass index (BMI) < 18.5 kg/m2 or ≥ 30 kg/m2, respectively). We aim to use survival analysis to identify an optimal body size indexation metric for echocardiographic measures that would be a better predictor of survival than BSA regardless of BMI. Adult patients with no prior valve replacement were selected from the National Echocardiography Database Australia. Survival analysis was performed for echocardiographic measures both unindexed and indexed to different body size metrics, with 5-year cardiovascular mortality as the primary endpoint. Indexation of echocardiographic measures (left ventricular end-diastolic diameter [n = 230,109] and mass [n = 224,244], left atrial volume [n = 150,540], aortic sinus diameter [n = 90,805], right atrial area [n = 59,516]) by BSA had better prognostic performance vs unindexed measures (underweight: C-statistic 0.655 vs 0.647; normal weight/overweight: average C-statistic 0.666 vs 0.625; obese: C-statistic 0.627 vs 0.613). Indexation by other body size metrics (lean body mass, height, and/or weight raised to different powers) did not improve prognostic performance versus BSA by a clinically relevant magnitude (average C-statistic increase ≤ 0.02), with smaller differences in other BMI subgroups. Indexing measures of cardiac and aortic size by BSA improves prognostic performance regardless of BMI, and no other body size metric has a clinically meaningful better performance.
© 2023. The Author(s).
Conflict of interest statement
D.P. has received modest honorarium from Alerte Echo IQ. The study was funded in part by grants to M.U. from New South Wales Health, Heart Research Australia, and the University of Sydney. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
