

ERK1/2 Phosphorylation Predicts Survival in Recurrent Glioblastoma Following Intracerebral and Adjuvant PD-1/CTLA-4 Immunotherapy: A REMARK-guided Analysis
- PMID: 37939133
- PMCID: PMC10842826
- DOI: 10.1158/1078-0432.CCR-23-1889
ERK1/2 Phosphorylation Predicts Survival in Recurrent Glioblastoma Following Intracerebral and Adjuvant PD-1/CTLA-4 Immunotherapy: A REMARK-guided Analysis
Abstract
Purpose: Evidence suggests that MAPK pathway activation, as measured by ERK1/2 phosphorylation (p-ERK), predicts overall survival (OS) in patients with recurrent glioblastoma receiving anti-PD-1 therapy. We aimed to validate these findings in independent cohorts.
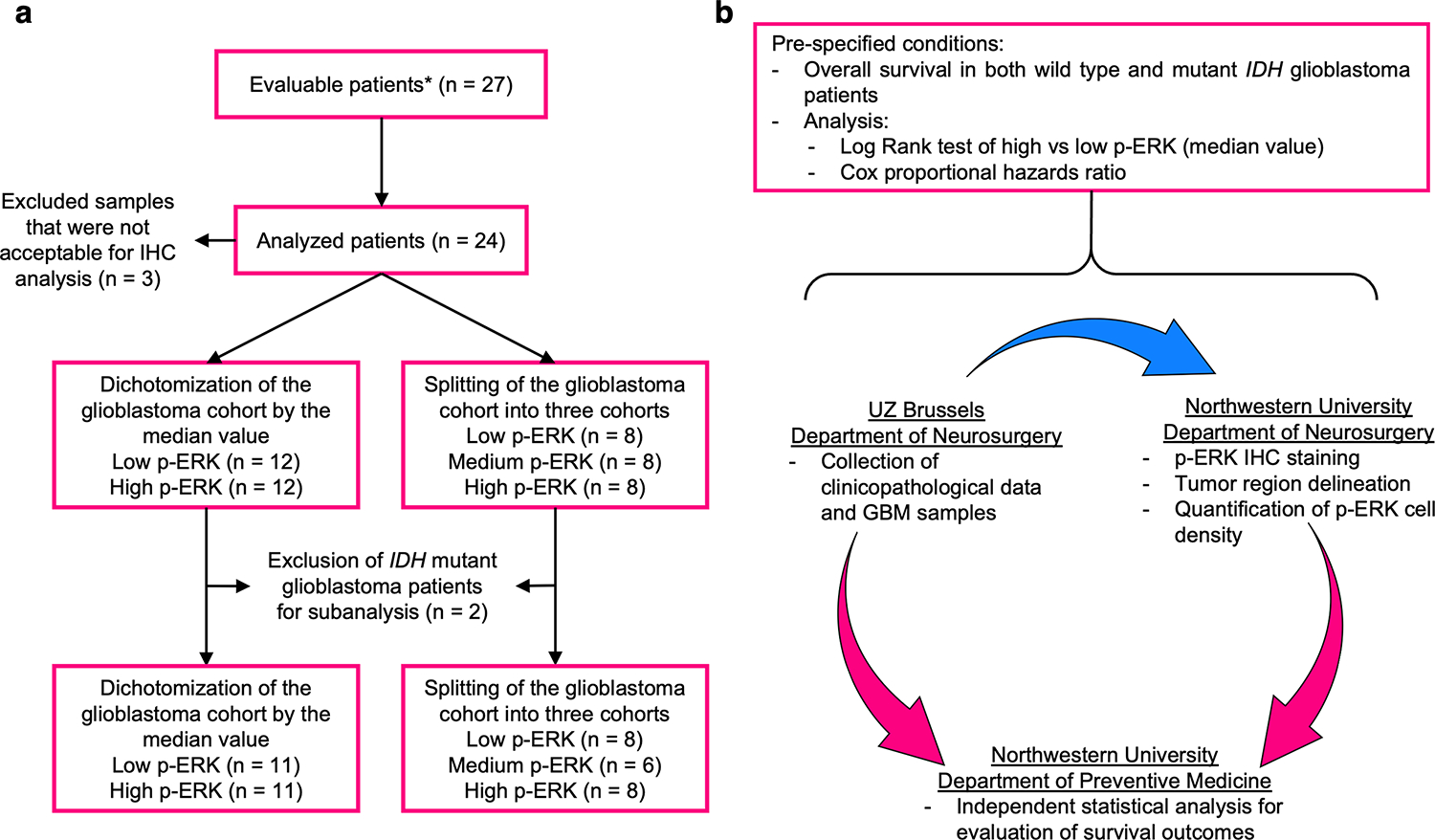
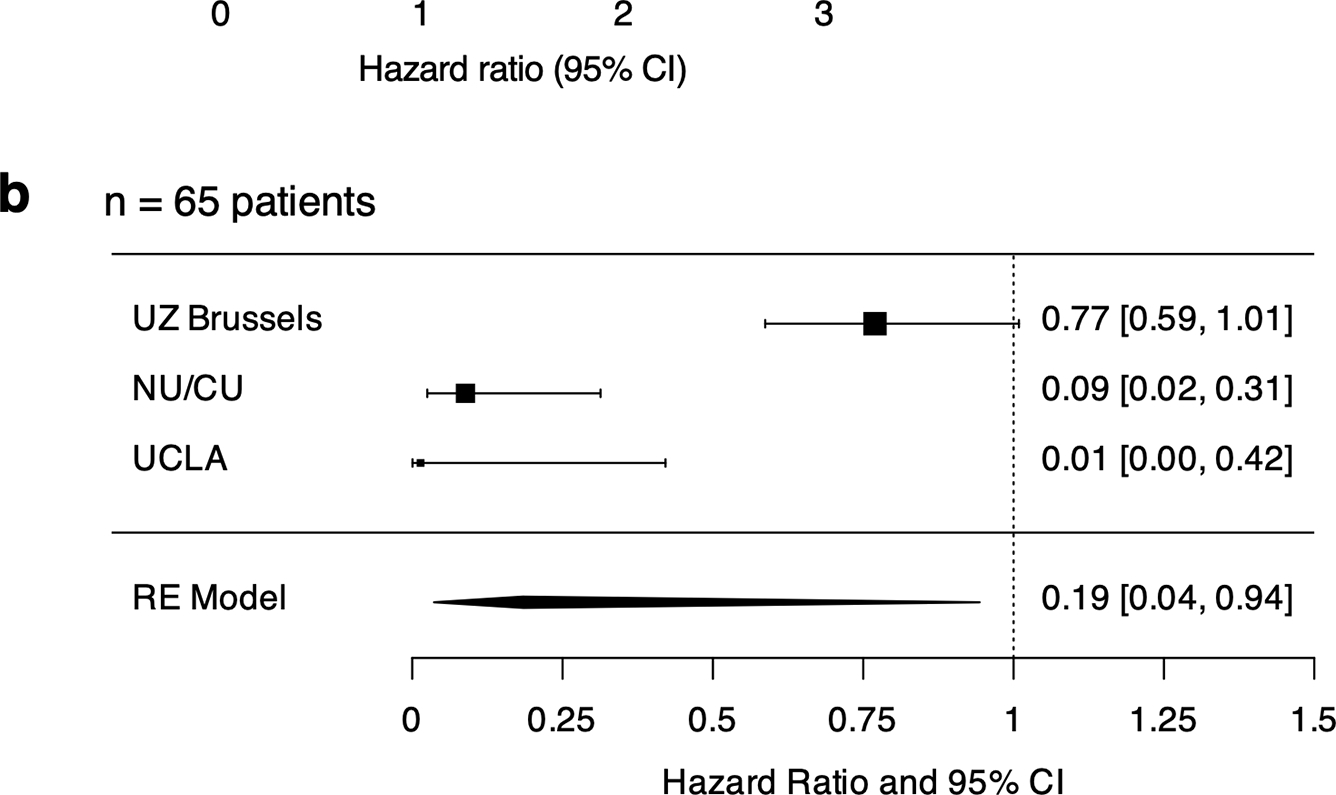
Experimental design: In a 24-patient clinical trial on recurrent glioblastoma and high-grade gliomas, we examined the link between p-ERK levels and OS. Patients received intravenous nivolumab, followed by maximal safe resection and an intracerebral injection of either ipilimumab alone or combined with nivolumab. Biweekly adjuvant nivolumab was then administered up to five times (NCT03233152). Using REporting recommendations for tumor MARKER prognostic studies (REMARK) criteria, we conducted independent analyses for p-ERK quantification and statistical evaluations. Additional comparative analysis included prior cohorts, totaling 65 patients. Cox proportional hazards models and meta-analysis were employed to assess p-ERK as a predictive biomarker after immunotherapy.
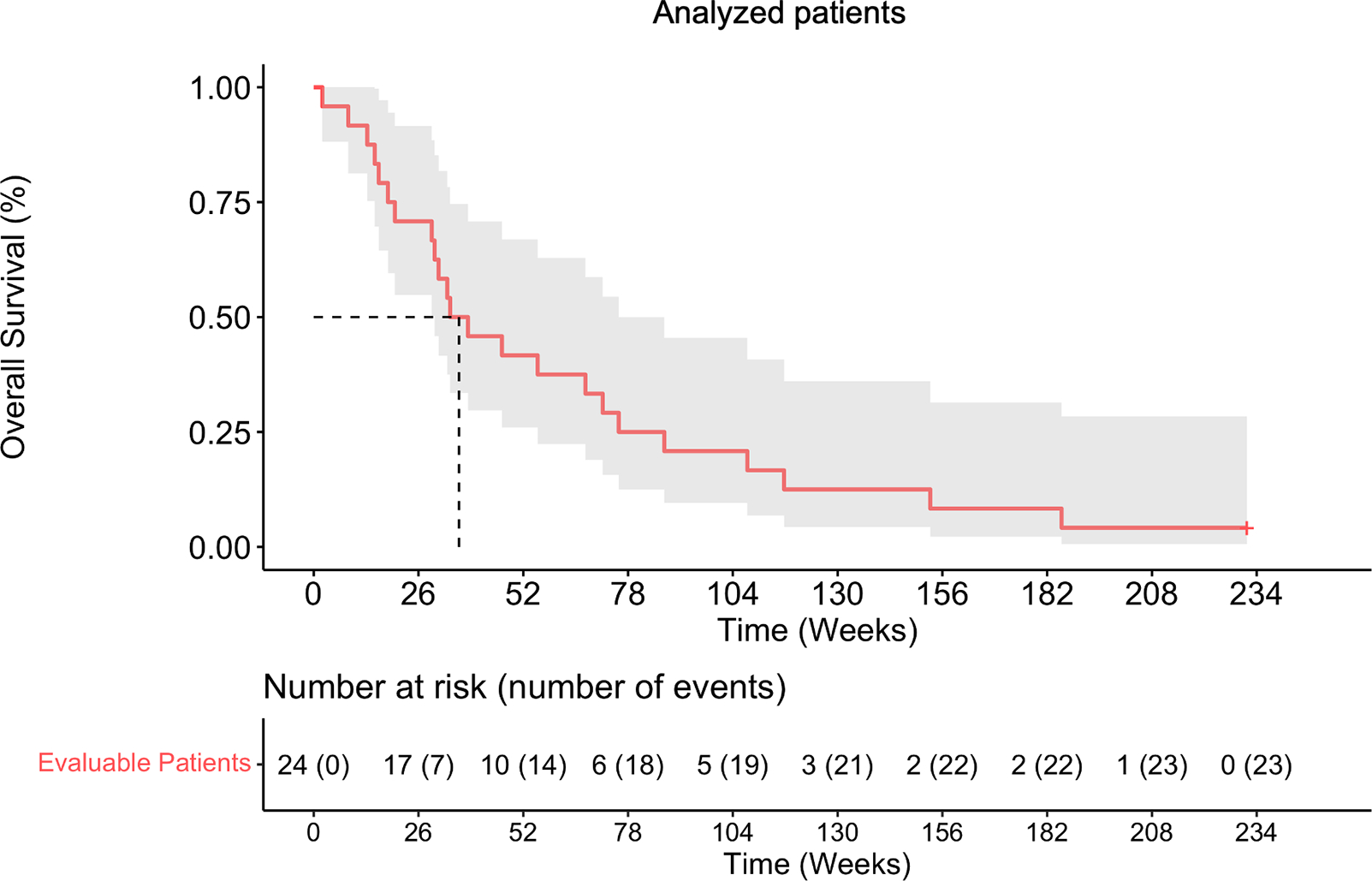
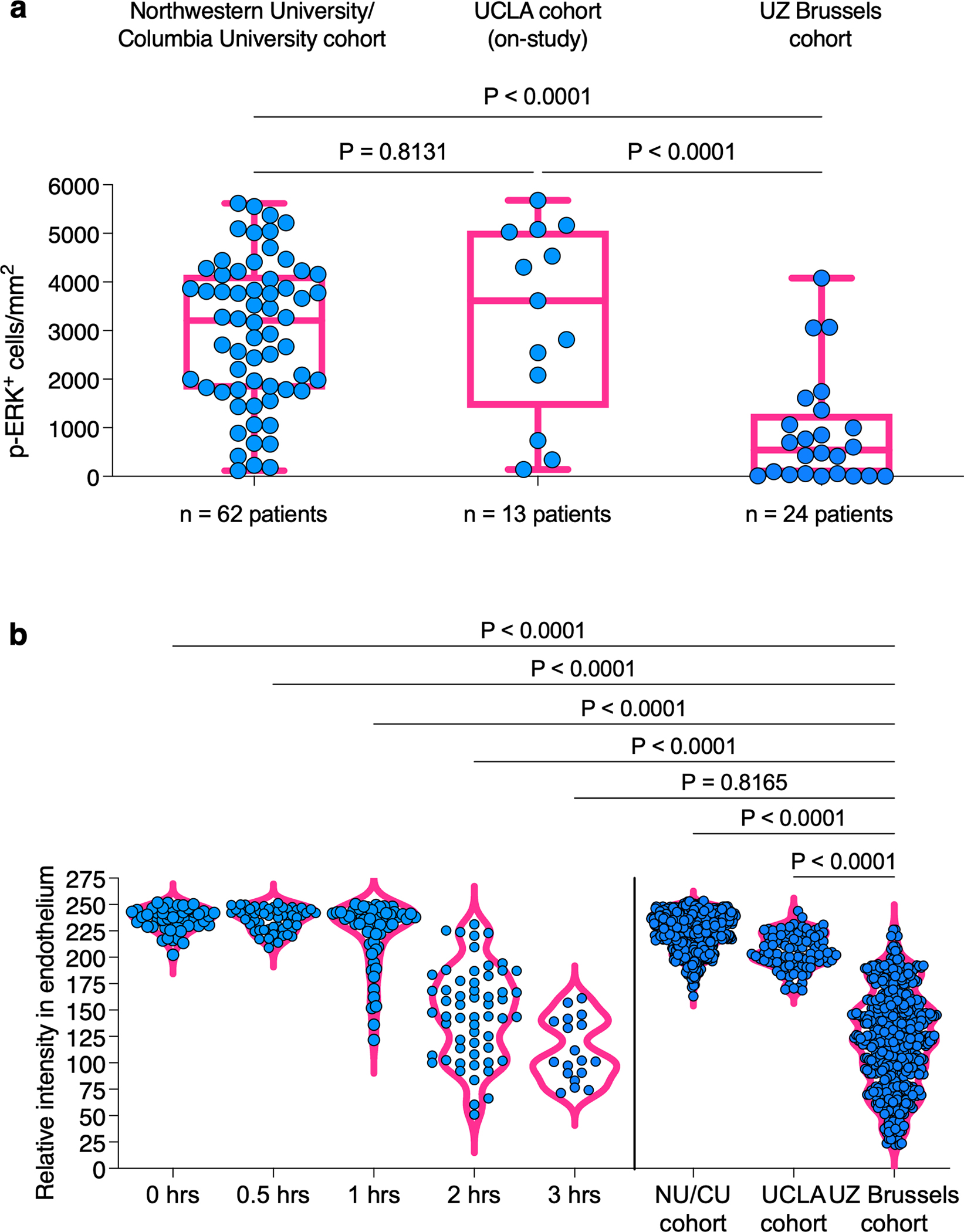
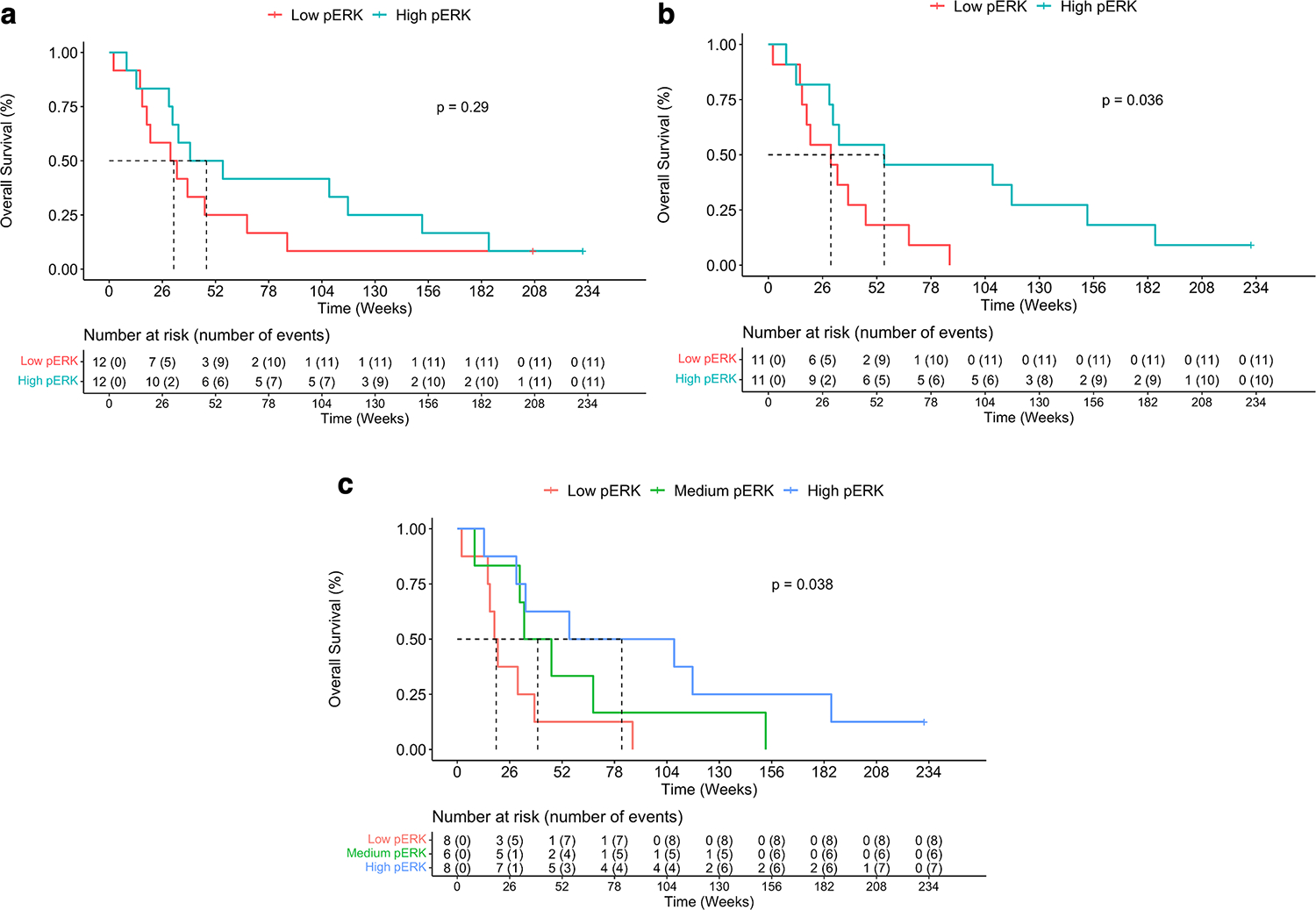
Results: Lower median p-ERK+ cell density was observed compared with prior studies, likely due to variable tissue processing across cohorts. Nonetheless, high p-ERK was associated with prolonged OS, particularly in isocitrate dehydrogenase wild-type glioblastomas (P = 0.036). Median OS for high and low p-ERK patients were 55.6 and 30 weeks, respectively. Multivariable analysis reinforced p-ERK's significance in survival prediction (P = 0.011). Upon p-ERK normalization across cohorts (n = 65), meta-analysis supported the survival benefit of elevated tumor p-ERK levels (P = 0.0424).
Conclusions: This study strengthens the role of p-ERK as a predictive biomarker for OS in patients with glioblastoma on immune checkpoint blockade. Future research should focus on further validation in prospective trials and the standardization of preanalytical variables influencing p-ERK quantification.
©2023 American Association for Cancer Research.
Conflict of interest statement
CONFLICT OF INTEREST
Please refer to the COI declared by individual authors on the ICMJE forms submitted.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
