

Bayesian methods: a potential path forward for sepsis trials
- PMID: 37940985
- PMCID: PMC10634134
- DOI: 10.1186/s13054-023-04717-x
Bayesian methods: a potential path forward for sepsis trials
Erratum in
-
Correction to: Bayesian methods: a potential path forward for sepsis trials.Crit Care. 2024 Jan 3;28(1):11. doi: 10.1186/s13054-023-04791-1. Crit Care. 2024. PMID: 38172963 Free PMC article. No abstract available.
Abstract
Background: Given the success of recent platform trials for COVID-19, Bayesian statistical methods have become an option for complex, heterogenous syndromes like sepsis. However, study design will require careful consideration of how statistical power varies using Bayesian methods across different choices for how historical data are incorporated through a prior distribution and how the analysis is ultimately conducted. Our objective with the current analysis is to assess how different uses of historical data through a prior distribution, and type of analysis influence results of a proposed trial that will be analyzed using Bayesian statistical methods.
Methods: We conducted a simulation study incorporating historical data from a published multicenter, randomized clinical trial in the US and Canada of polymyxin B hemadsorption for treatment of endotoxemic septic shock. Historical data come from a 179-patient subgroup of the previous trial of adult critically ill patients with septic shock, multiple organ failure and an endotoxin activity of 0.60-0.89. The trial intervention consisted of two polymyxin B hemoadsorption treatments (2 h each) completed within 24 h of enrollment.
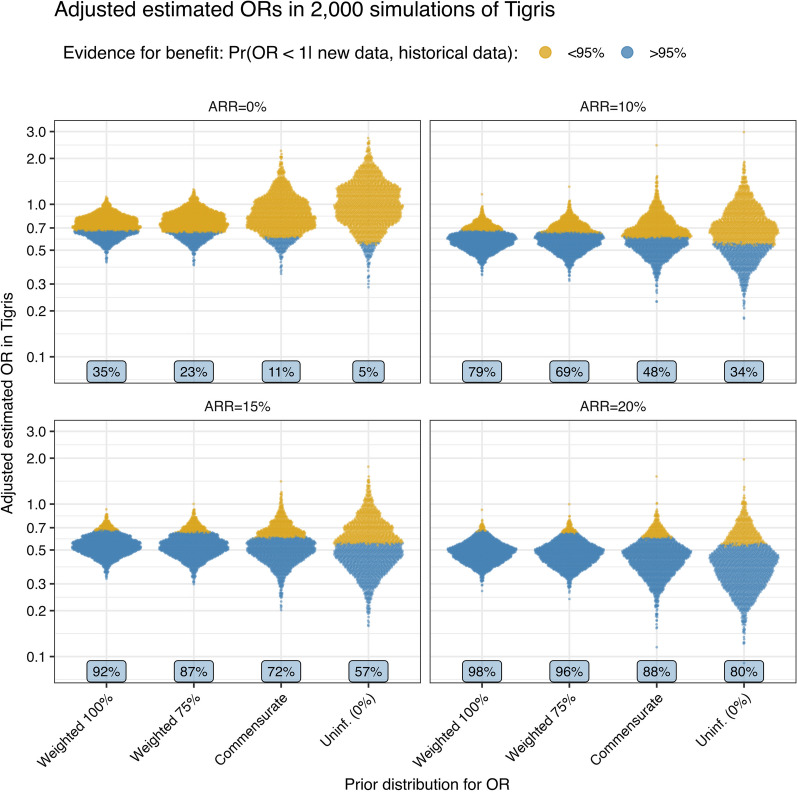
Results: In our simulations for a new trial of 150 patients, a range of hypothetical results were observed. Across a range of baseline risks and treatment effects and four ways of including historical data, we demonstrate an increase in power with the use of clinically defensible incorporation of historical data. In one possible trial result, for example, with an observed reduction in risk of mortality from 44 to 37%, the probability of benefit is 96% with a fixed weight of 75% on prior data and 90% with a commensurate (adaptive-weighting) prior; the same data give an 80% probability of benefit if historical data are ignored.
Conclusions: Using Bayesian methods and a biologically justifiable use of historical data in a prior distribution yields a study design with higher power than a conventional design that ignores relevant historical data. Bayesian methods may be a viable option for trials in critical care medicine where beneficial treatments have been elusive.
Keywords: Endotoxemia; Endotoxin septic shock; Hemadsorption; Polymyxin-B; Septic shock; Statistical methods; Trial simulation.
© 2023. The Author(s).
Conflict of interest statement
GT is a paid consultant to Spectral Medical. DMF, and JAK are employees of Spectral Medical. PMW is a member of the Board of Directors of Spectral Medical. AA-K, SAC, FNF, CG, KG, SK, RK-S, PM, NKM, RGP, J-SR, RR, MS and MT are/were investigators in the Tigris and/or EUPHRATES trials and their institutions received funding to conduct the studies.
Figures


References
-
- Yarnell CJ, Abrams D, Baldwin MR, Brodie D, Fan E, Ferguson ND, Hua M, Madahar P, McAuley DF, Munshi L, et al. Clinical trials in critical care: can a Bayesian approach enhance clinical and scientific decision making? Lancet Respir Med. 2021;9(2):207–216. doi: 10.1016/S2213-2600(20)30471-9. - DOI - PMC - PubMed
-
- Racine A, Grieve AP, Flühler H, Smith AF. Bayesian methods in practice: experiences in the pharmaceutical industry. Appl Stat. 1986;35:93–150. doi: 10.2307/2347264. - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
