

Cardiac amyloidosis and aortic stenosis: a state-of-the-art review
- PMID: 37941729
- PMCID: PMC10630099
- DOI: 10.1093/ehjopen/oead106
Cardiac amyloidosis and aortic stenosis: a state-of-the-art review
Abstract
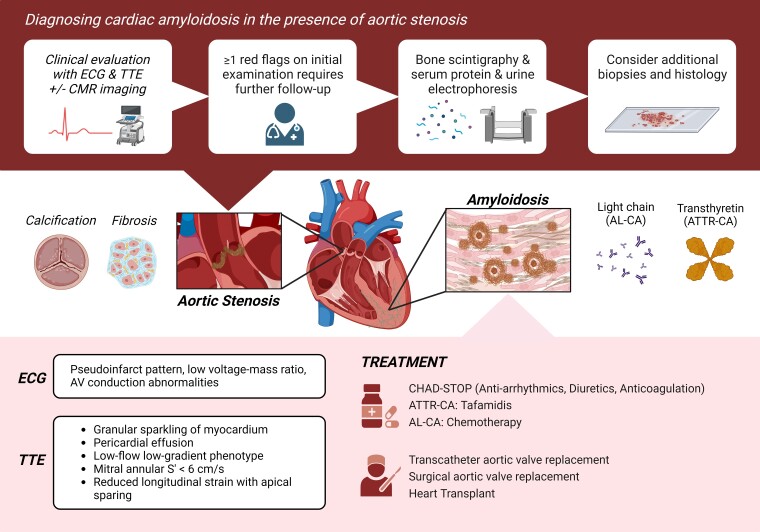
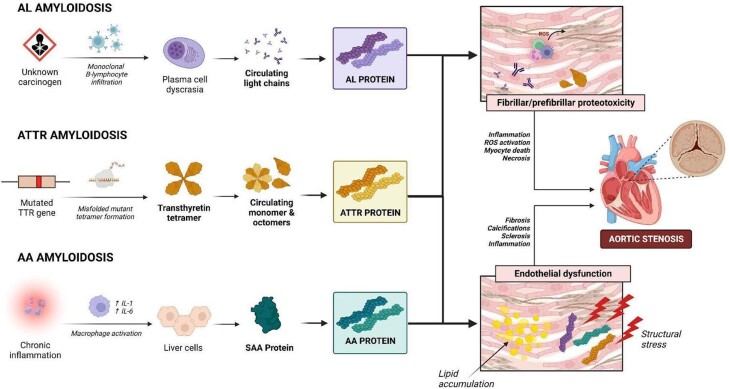
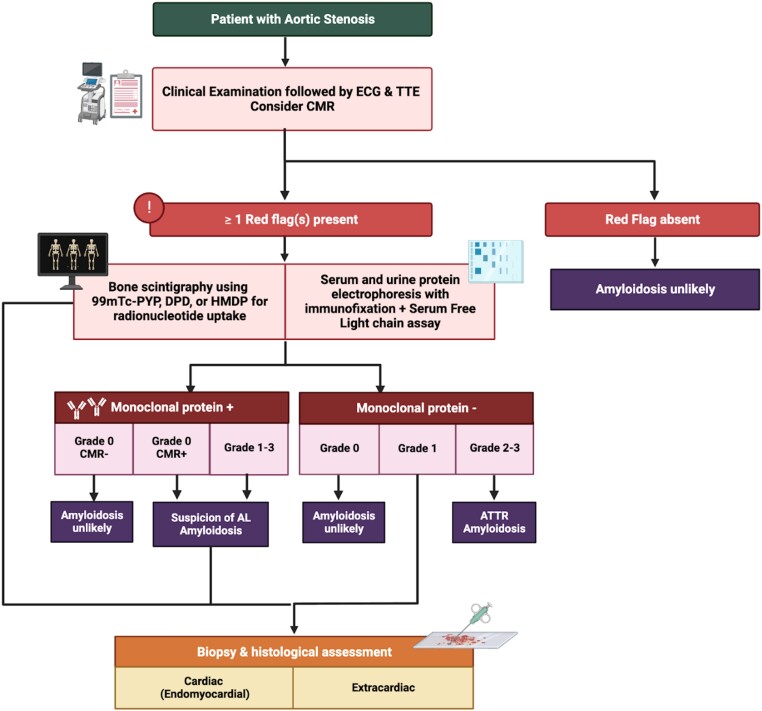
Cardiac amyloidosis is caused by the extracellular deposition of amyloid fibrils in the heart, involving not only the myocardium but also any cardiovascular structure. Indeed, this progressive infiltrative disease also involves the cardiac valves and, specifically, shows a high prevalence with aortic stenosis. Misfolded protein infiltration in the aortic valve leads to tissue damage resulting in the onset or worsening of valve stenosis. Transthyretin cardiac amyloidosis and aortic stenosis coexist in patients > 65 years in about 4-16% of cases, especially in those undergoing transcatheter aortic valve replacement. Diagnostic workup for cardiac amyloidosis in patients with aortic stenosis is based on a multi-parametric approach considering clinical assessment, electrocardiogram, haematologic tests, basic and advanced echocardiography, cardiac magnetic resonance, and technetium labelled cardiac scintigraphy like technetium-99 m (99mTc)-pyrophosphate, 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid, and 99mTc-hydroxymethylene diphosphonate. However, a biopsy is the traditional gold standard for diagnosis. The prognosis of patients with coexisting cardiac amyloidosis and aortic stenosis is still under evaluation. The combination of these two pathologies worsens the prognosis. Regarding treatment, mortality is reduced in patients with cardiac amyloidosis and severe aortic stenosis after undergoing transcatheter aortic valve replacement. Further studies are needed to confirm these findings and to understand whether the diagnosis of cardiac amyloidosis could affect therapeutic strategies. The aim of this review is to critically expose the current state-of-art regarding the association of cardiac amyloidosis with aortic stenosis, from pathophysiology to treatment.
Keywords: Aortic stenosis; Cardiac amyloidosis; Cardiomyopathy; Diagnosis.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: A.G. is currently working as Editor of European Heart Journal Cardiovascular Imaging, EHJ Open, and Editor in Chief of EHJ Imaging Methods and Practice. S.D.R. is currently working as section Editor in European Heart Journal Open. K.J.G. serves as an advisor for Medtronic, Abbott, and Boston Scientific and is a speaker for Edwards Lifesciences.
Figures
References
-
- Balciunaite G, Rimkus A, Zurauskas E, Zaremba T, Palionis D, Valeviciene N, Aidietis A, Serpytis P, Rucinskas K, Sogaard P, Glaveckaite S, Zorinas A, Janusauskas V. Transthyretin cardiac amyloidosis in aortic stenosis: prevalence, diagnostic challenges, and clinical implications. Hellenic J Cardiol 2020;61:92–98. - PubMed
-
- Barrett CD, Dobos K, Liedtke M, Tuzovic M, Haddad F, Kobayashi Y, Lafayette R, Fowler MB, Arai S, Schrier S, Witteles RM. A changing landscape of mortality for systemic light chain amyloidosis. JACC Heart Fail 2019;7:958–966. - PubMed
-
- Kenchaiah S, Pfeffer MA. Cardiac remodeling in systemic hypertension. Med Clin North Am 2004;88:115–130. - PubMed
-
- Ross J, Braunwald E. Aortic stenosis. Circulation 1968;38:61–67. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
