

Reproducible and Effective Biceps Tenodesis Method Utilizing In-Office Nano-Arthroscopy
- PMID: 37942114
- PMCID: PMC10628057
- DOI: 10.1016/j.eats.2023.06.009
Reproducible and Effective Biceps Tenodesis Method Utilizing In-Office Nano-Arthroscopy
Abstract
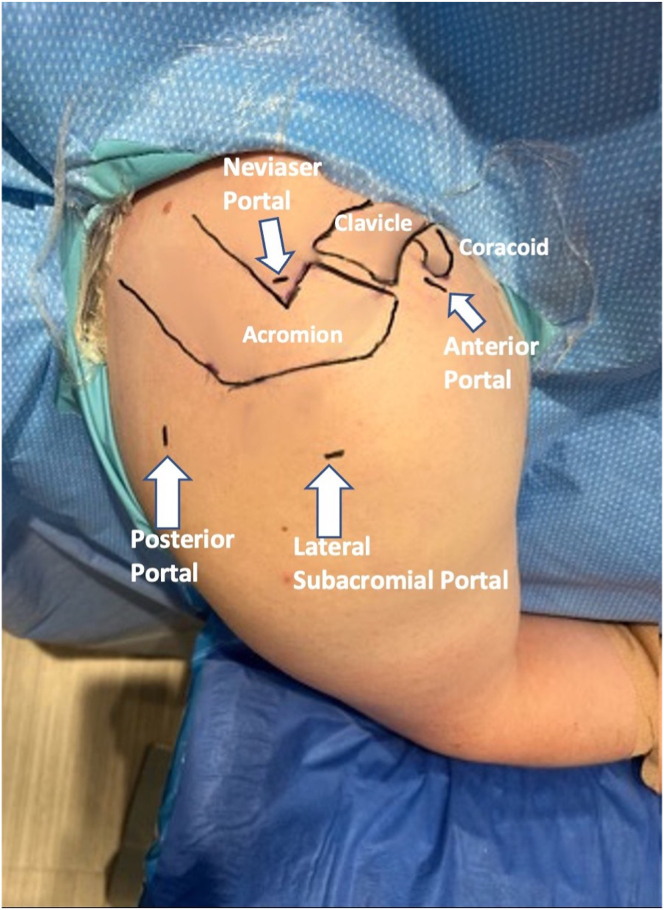
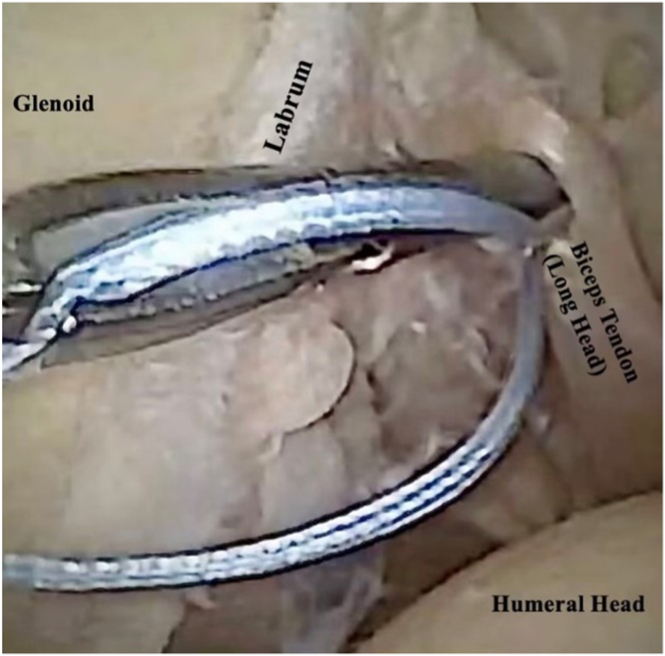
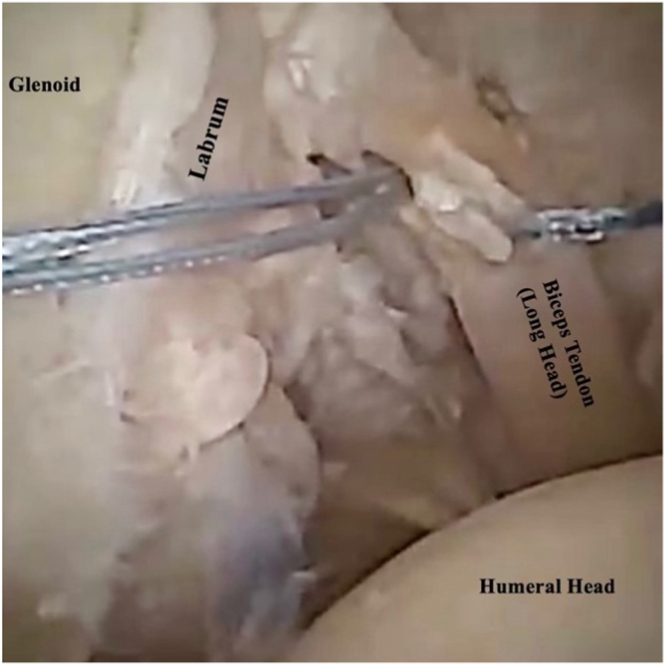
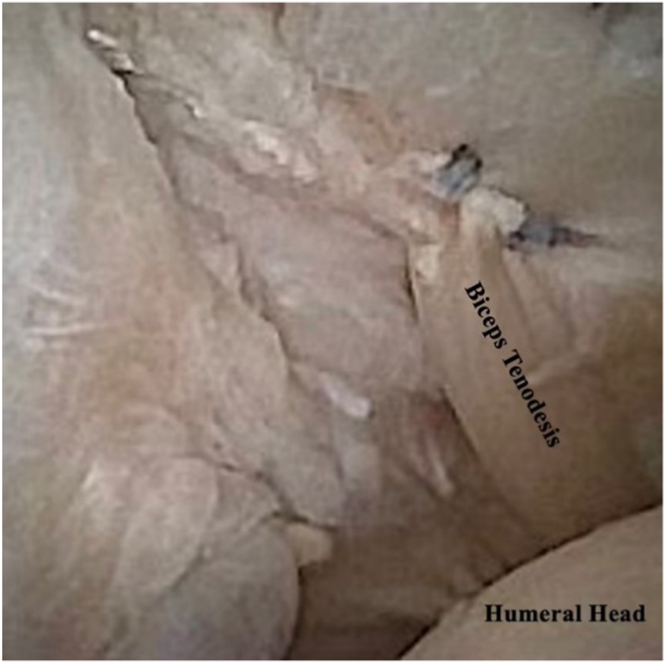
Biceps tendinopathy is a common cause of chronic anterior shoulder pain characterized by altered joint mechanics with considerable deficits in range of motion secondary to pain. The benefits of in-office nano-arthroscopy (IONA) include the ability to diagnosis and treat biceps tendinopathy, quicker patient recovery, reduced cost, and improved patient satisfaction. The purpose of this technical report is to describe the technique for performing IONA for biceps tendinopathy (biceps tenotomy/biceps tenodesis), with special consideration for obtaining adequate local anesthesia, proper indications, adequate visualization, and the advantages of performing these procedures in the office rather than the operating room.
© 2023 The Authors.
Figures

References
-
- Wilk K.E., Hooks T.R. The Painful long head of the biceps brachii: Nonoperative treatment approaches. Clin Sports Med. 2016;35:75–92. - PubMed
-
- Hsu A.R., Ghodadra N.S., Provencher M.T., Lewis P.B., Bach B.R. Biceps tenotomy versus tenodesis: A review of clinical outcomes and biomechanical results. J Shoulder Elbow Surg. 2011;20:326–332. - PubMed
-
- Castricini R., Familiari F., De Gori M., et al. Tenodesis is not superior to tenotomy in the treatment of the long head of biceps tendon lesions. Knee Surg Sports Traumatol Arthrosc. 2018;26:169–175. - PubMed
-
- Belk J.W., Kraeutler M.J., Houck D.A., Chrisman A.N., Scillia A.J., McCarty E.C. Biceps tenodesis versus tenotomy: A systematic review and meta-analysis of level I randomized controlled trials. J Shoulder Elbow Surg. 2021;30:951–960. - PubMed
-
- Golish S.R., Caldwell P.E., III, Miller M.D., et al. Interference screw versus suture anchor fixation for subpectoral tenodesis of the proximal biceps tendon: A cadaveric study. Arthroscopy. 2008;24:1103–1108. - PubMed
LinkOut - more resources
Full Text Sources
