

Practice Patterns for Organ Preservation in US Patients With Rectal Cancer, 2006-2020
- PMID: 37943566
- PMCID: PMC10636650
- DOI: 10.1001/jamaoncol.2023.4845
Practice Patterns for Organ Preservation in US Patients With Rectal Cancer, 2006-2020
Abstract
Importance: In March 2023, the National Comprehensive Cancer Network endorsed watch and wait for those with complete clinical response to total neoadjuvant therapy. Neoadjuvant therapy is highly efficacious, so this recommendation may have broad implications, but the current trends in organ preservation in the US are unknown.
Objective: To describe organ preservation trends among patients with rectal cancer in the US from 2006 to 2020.
Design, setting, and participants: This retrospective, observational case series included adults (aged ≥18 years) with rectal adenocarcinoma managed with curative intent from 2006 to 2020 in the National Cancer Database.
Exposure: The year of treatment was the primary exposure. The type of therapy was chemotherapy, radiation, or surgery (proctectomy, transanal local excision, no tumor resection). The timing of therapy was classified as neoadjuvant or adjuvant.
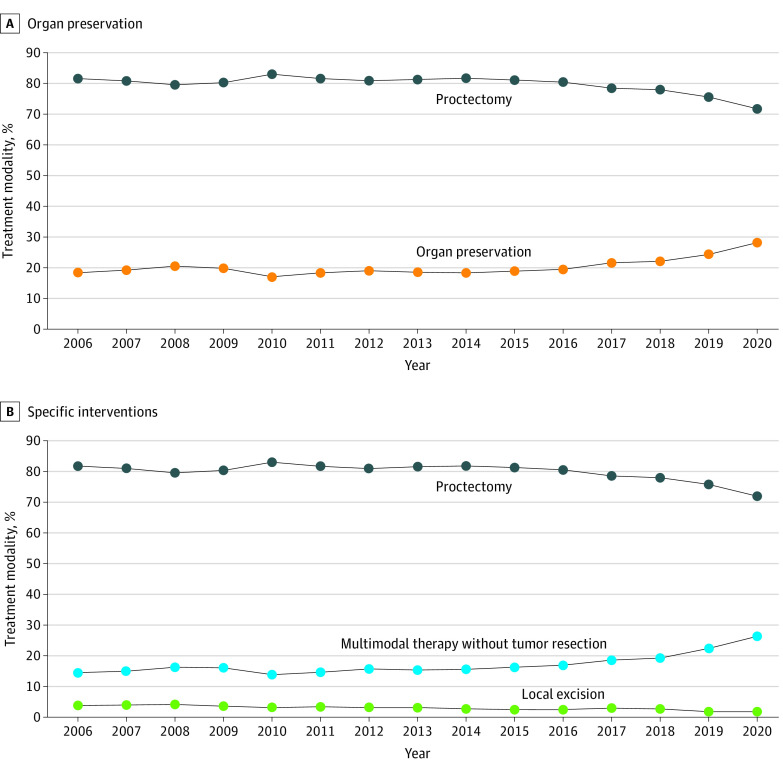
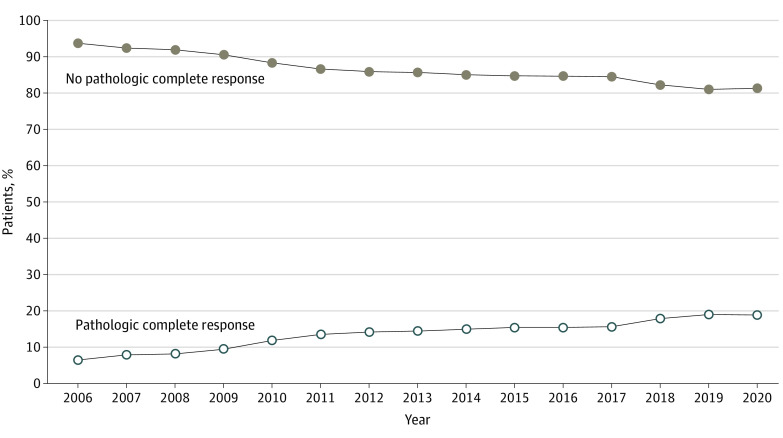
Main outcomes and measures: The primary outcome was the absolute annual proportion of organ preservation after radical treatment, defined as chemotherapy and/or radiation without tumor resection, proctectomy, or transanal local excision. A secondary analysis examined complete pathologic responses among eligible patients.
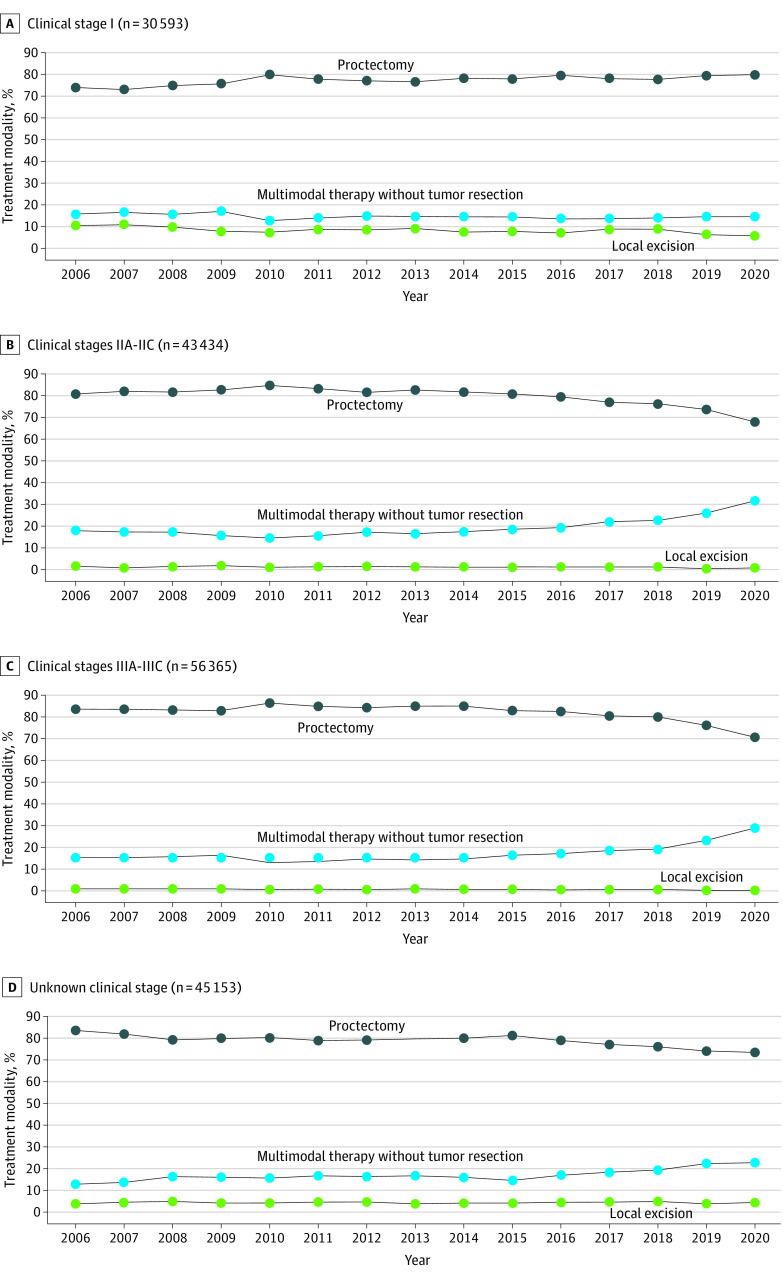
Results: Of the 175 545 patients included, the mean (SD) age was 63 (13) years, 39.7% were female, 17.4% had clinical stage I disease, 24.7% had stage IIA to IIC disease, 32.1% had stage IIIA to IIIC disease, and 25.7% had unknown stage. The absolute annual proportion of organ preservation increased by 9.8 percentage points (from 18.4% in 2006 to 28.2% in 2020; P < .001). From 2006 to 2020, the absolute rate of organ preservation increased by 13.0 percentage points for patients with stage IIA to IIC disease (19.5% to 32.5%), 12.9 percentage points for patients with stage IIIA to IIC disease (16.2% to 29.1%), and 10.1 percentage points for unknown stages (16.5% to 26.6%; all P < .001). Conversely, patients with stage I disease experienced a 6.1-percentage point absolute decline in organ preservation (from 26.4% in 2006 to 20.3% in 2020; P < .001). The annual rate of transanal local excisions decreased for all stages. In the subgroup of 80 607 eligible patients, the proportion of complete pathologic responses increased from 6.5% in 2006 to 18.8% in 2020 (P < .001).
Conclusions and relevance: This case series shows that rectal cancer is increasingly being managed medically, especially among patients whose treatment historically relied on proctectomy. Given the National Comprehensive Cancer Network endorsement of watch and wait, the increasing trends in organ preservation, and the nearly 3-fold increase in complete pathologic responses, international professional societies should urgently develop multidisciplinary core outcome sets and care quality indicators to ensure high-quality rectal cancer research and care delivery accounting for organ preservation.
Conflict of interest statement
Figures
References
-
- Peeters KC, van de Velde CJ, Leer JW, et al. Late side effects of short-course preoperative radiotherapy combined with total mesorectal excision for rectal cancer: increased bowel dysfunction in irradiated patients—a Dutch colorectal cancer group study. J Clin Oncol. 2005;23(25):6199-6206. doi: 10.1200/JCO.2005.14.779 - DOI - PubMed
-
- NCCN Clinical Practice Guidelines in Oncology: rectal cancer. National Comprehensive Cancer Network . July 25, 2023. Accessed July 29, 2023. https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf - PubMed
-
- van der Valk MJM, Hilling DE, Bastiaannet E, et al. ; IWWD Consortium . Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): an international multicentre registry study. Lancet. 2018;391(10139):2537-2545. doi: 10.1016/S0140-6736(18)31078-X - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
