

Preclinical Evaluation of Minigastrin Analogs and Proof-of-Concept [68Ga]Ga-DOTA-CCK-66 PET/CT in 2 Patients with Medullary Thyroid Cancer
- PMID: 37945383
- PMCID: PMC10755518
- DOI: 10.2967/jnumed.123.266537
Preclinical Evaluation of Minigastrin Analogs and Proof-of-Concept [68Ga]Ga-DOTA-CCK-66 PET/CT in 2 Patients with Medullary Thyroid Cancer
Abstract
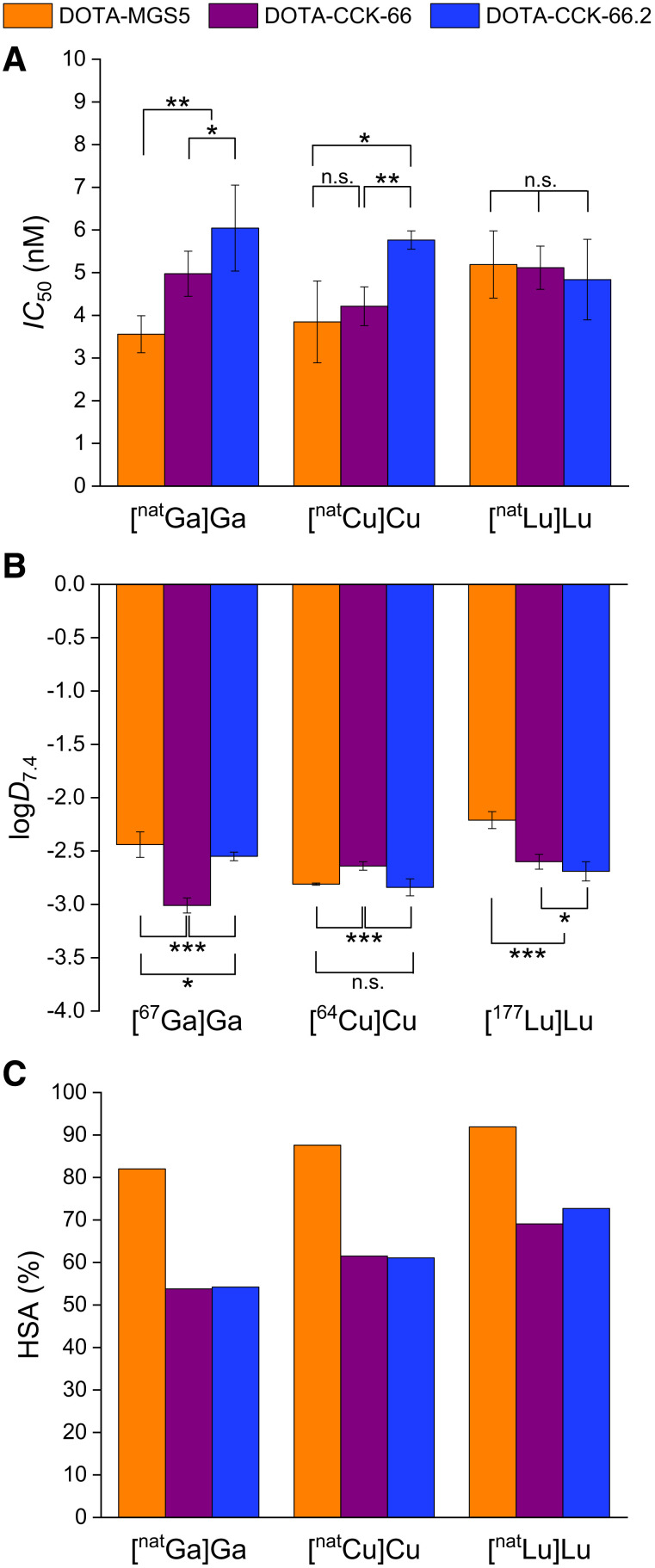
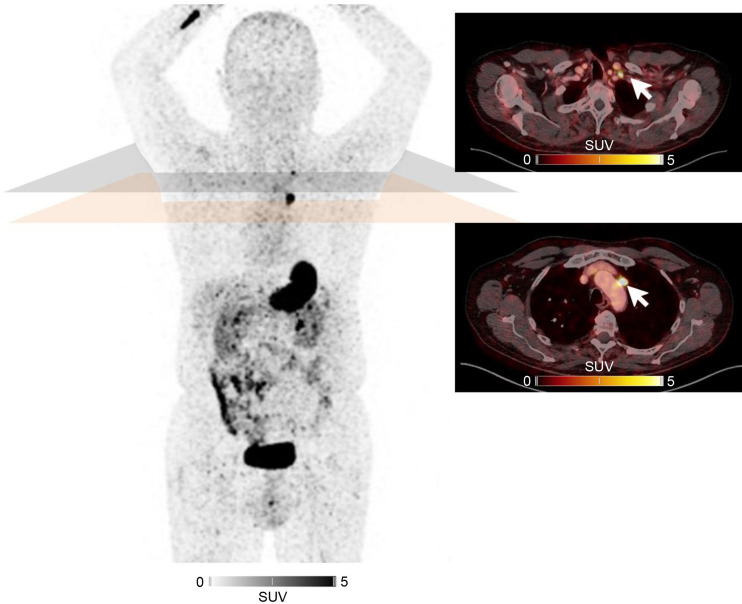
Because of the need for radiolabeled theranostics for the detection and treatment of medullary thyroid cancer (MTC), and the yet unresolved stability issues of minigastrin analogs targeting the cholecystokinin-2 receptor (CCK-2R), our aim was to address in vivo stability, our motivation being to develop and evaluate DOTA-CCK-66 (DOTA-γ-glu-PEG3-Trp-(N-Me)Nle-Asp-1-Nal-NH2, PEG: polyethylene glycol) and DOTA-CCK-66.2 (DOTA-glu-PEG3-Trp-(N-Me)Nle-Asp-1-Nal-NH2), both derived from DOTA-MGS5 (DOTA-glu-Ala-Tyr-Gly-Trp-(N-Me)Nle-Asp-1-Nal-NH2), and clinically translate [68Ga]Ga-DOTA-CCK-66. Methods: 64Cu and 67Ga labeling of DOTA-CCK-66, DOTA-CCK-66.2, and DOTA-MGS5 was performed at 90°C within 15 min (1.0 M NaOAc buffer, pH 5.5, and 2.5 M 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid buffer, respectively). 177Lu labeling of these 3 compounds was performed at 90°C within 15 min (1.0 M NaOAc buffer, pH 5.5, 0.1 M sodium ascorbate). CCK-2R affinity of natGa/natCu/natLu-labeled DOTA-CCK-66, DOTA-CCK-66.2, and DOTA-MGS5 was examined on AR42J cells. The in vivo stability of 177Lu-labeled DOTA-CCK-66 and DOTA-MGS5 was examined at 30 min after injection in CB17-SCID mice. Biodistribution studies at 1 h ([67Ga]Ga-DOTA-CCK-66) and 24 h ([177Lu]Lu-DOTA-CCK-66/DOTA-MGS5) after injection were performed on AR42J tumor-bearing CB17-SCID mice. In a translation to the human setting, [68Ga]Ga-DOTA-CCK-66 was administered and whole-body PET/CT was acquired at 120 min after injection in 2 MTC patients. Results: Irrespective of the metal or radiometal used (copper, gallium, lutetium), high CCK-2R affinity (half-maximal inhibitory concentration, 3.6-6.0 nM) and favorable lipophilicity were determined. In vivo, increased numbers of intact peptide were found for [177Lu]Lu-DOTA-CCK-66 compared with [177Lu]Lu-DOTA-MGS5 in murine urine (23.7% ± 9.2% vs. 77.8% ± 2.3%). Overall tumor-to-background ratios were similar for both 177Lu-labeled analogs. [67Ga]Ga-DOTA-CCK-66 exhibited accumulation (percentage injected dose per gram) that was high in tumor (19.4 ± 3.5) and low in off-target areas (blood, 0.61 ± 0.07; liver, 0.31 ± 0.02; pancreas, 0.23 ± 0.07; stomach, 1.81 ± 0.19; kidney, 2.51 ± 0.49) at 1 h after injection. PET/CT examination in 2 MTC patients applying [68Ga]Ga-DOTA-CCK-66 confirmed multiple metastases. Conclusion: Because of the high in vivo stability and favorable overall preclinical performance of [nat/67Ga]Ga-/[nat/177Lu]Lu-DOTA-CCK-66, a proof-of-concept clinical investigation of [68Ga]Ga-DOTA-CCK-66 was completed. As several lesions could be identified and excellent biodistribution patterns were observed, further patient studies applying [68Ga]Ga- and [177Lu]Lu-DOTA-CCK-66 are warranted.
Keywords: CCK-2R; DOTA-CCK-66; clinical translation; medullary thyroid cancer.
© 2024 by the Society of Nuclear Medicine and Molecular Imaging.
Figures





References
-
- Thyroid cancer: statistics. Cancer.net website. https://www.cancer.net/cancer-types/thyroid-cancer/statistics#:∼:text=In.... Published August 2023. Accessed October 30, 2023.
-
- Roman S, Lin R, Sosa JA. Prognosis of medullary thyroid carcinoma: demographic, clinical, and pathologic predictors of survival in 1252 cases. Cancer. 2006;107:2134–2142. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous