

Genomic and immune signatures predict clinical outcome in newly diagnosed multiple myeloma treated with immunotherapy regimens
- PMID: 37945755
- PMCID: PMC12065606
- DOI: 10.1038/s43018-023-00657-1
Genomic and immune signatures predict clinical outcome in newly diagnosed multiple myeloma treated with immunotherapy regimens
Abstract
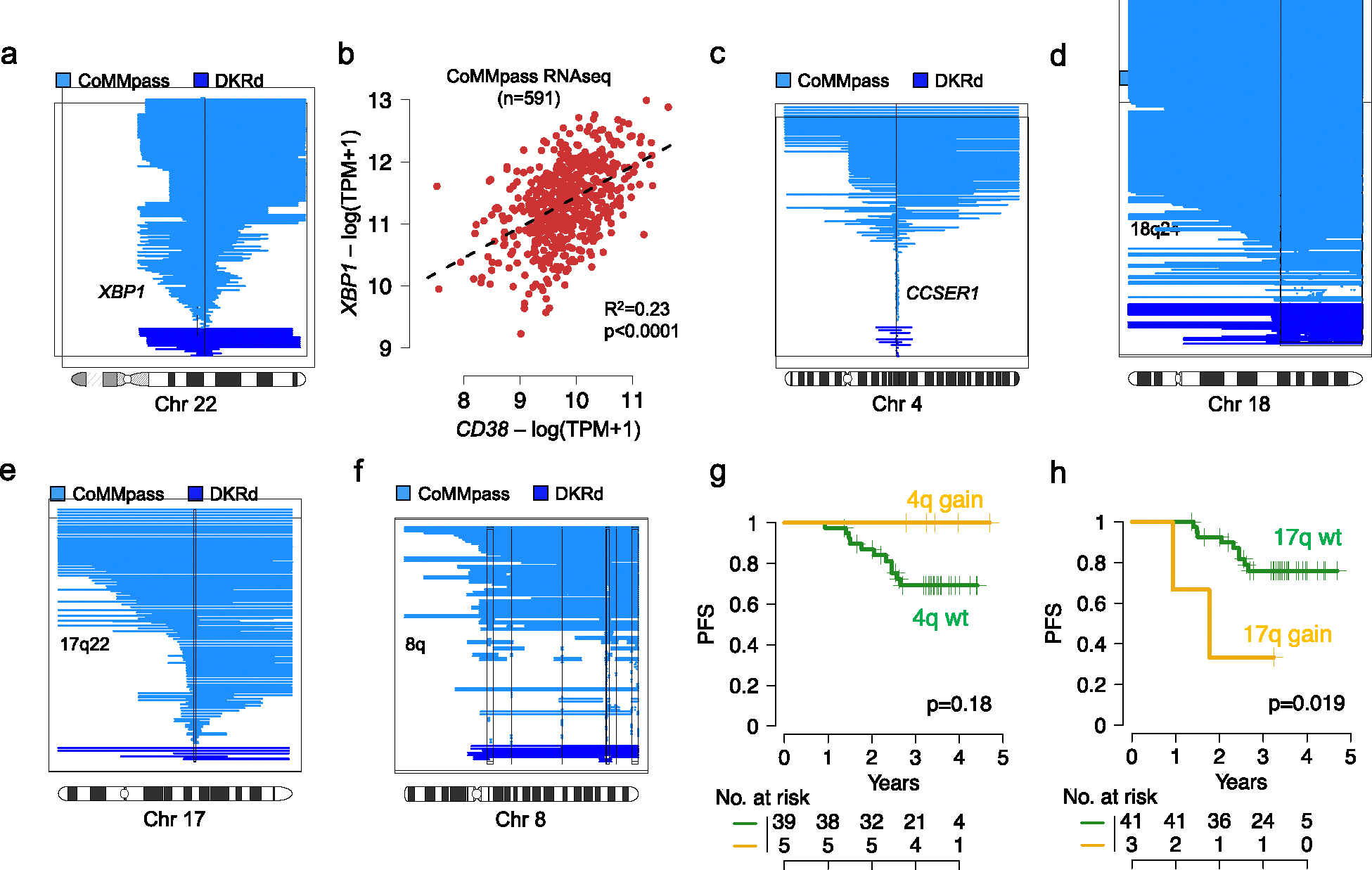
Despite improving outcomes, 40% of patients with newly diagnosed multiple myeloma treated with regimens containing daratumumab, a CD38-targeted monoclonal antibody, progress prematurely. By integrating tumor whole-genome and microenvironment single-cell RNA sequencing from upfront phase 2 trials using carfilzomib, lenalidomide and dexamethasone with daratumumab ( NCT03290950 ), we show how distinct genomic drivers including high APOBEC mutational activity, IKZF3 and RPL5 deletions and 8q gain affect clinical outcomes. Furthermore, evaluation of paired bone marrow profiles, taken before and after eight cycles of carfilzomib, lenalidomide and dexamethasone with daratumumab, shows that numbers of natural killer cells before treatment, high T cell receptor diversity before treatment, the disappearance of sustained immune activation (that is, B cells and T cells) and monocyte expansion over time are all predictive of sustained minimal residual disease negativity. Overall, this study provides strong evidence of a complex interplay between tumor cells and the immune microenvironment that is predictive of clinical outcome and depth of treatment response in patients with newly diagnosed multiple myeloma treated with highly effective combinations containing anti-CD38 antibodies.
© 2023. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
CONFLICT OF INTEREST STATEMENT
O.L. has received research funding from: National Institutes of Health (NIH), National Cancer Institute (NCI), U.S. Food and Drug Administration (FDA), Multiple Myeloma Research Foundation (MMRF), International Myeloma Foundation (IMF), Leukemia and Lymphoma Society (LLS), the Paula and Rodger Riney Myeloma Foundation, Tow Foundation, Myeloma Solutions Fund, Perelman Family Foundation, Rising Tide Foundation, Amgen, Celgene, Janssen, Takeda, Glenmark, Pfizer, Seattle Genetics, Karyopharm; Honoraria/ad boards: Adaptive, Amgen, Binding Site, BMS, Celgene, Cellectis, Glenmark, Janssen, Juno, Pfizer; and serves on Independent Data Monitoring Committees (IDMCs) for clinical trials lead by Takeda, Merck, Janssen, Theradex.
G.J.M. has received funding from National Institutes of Health (NIH), National Cancer Institute (NCI), Multiple Myeloma Research Foundation (MMRF), Leukemia and Lymphoma Society (LLS), Perelman Family Foundation, Amgen, Celgene, Janssen, Takeda; Honoraria/ad boards: Adaptive, Amgen, BMS, Celgene, Janssen; and serves on Independent Data Monitoring Committees (IDMCs) for clinical trials lead by Takeda, Karyopharm and Sanofi.
M.S.: Clinical trial research support to institution: Angiocrine Bioscience, Inc.; Omeros Corporation; Amgen, Inc. Consultancy: Omeros Corporation; Angiocrine Bioscience, Inc. (past); McKinsey & Company (past). Ad-hoc advisory board: Kite – A Gilead Company (past) CME activity honorarium: i3Health (past); Medscape, LLC. (past), CancerNetwork.
G.S.: research funding to the institution from Janssen, Amgen, BMS, and Beyond Spring. DSMB for Arcellx
S.G. receives research funding from Miltenyi Biotec, Takeda Pharmaceutical Co., Celgene Corp., Amgen Inc., Sanofi, Johnson and Johnson, Inc., Actinium Pharmaceuticals, Inc., and is on the Advisory Boards for: Kite Pharmaceuticals, Inc., Celgene Corp., Sanofi, Novartis, Johnson and Johnson, Inc., Amgen Inc., Takeda Pharmaceutical Co., Jazz Pharmaceuticals, Inc., Actinium Pharmaceuticals, Inc.
U.A.S. reports research funding support from Celgene/BMS, Janssen to the institution, non-financial research support; personal fees from ACCC, MashUp MD, Janssen Biotech, Sanofi, BMS, MJH LifeSciences, Intellisphere, Phillips Gilmore Oncology Communications, i3 Health and RedMedEd outside the submitted work.
S.U. Research funding: Abbvie, Amgen, Array Biopharma, BMS, Celgene, Gilead, GSK, Janssen, Merck, Pharmacyclics, Sanofi, Seattle Genetics, SkylineDX, Takeda. Advisory/Consulting: Abbvie, Amgen, BMS, Celgene, EdoPharma, Genentech, Gilead, GSK, Janssen, K36 Therapeutics, Moderna, Novartis, Oncopeptides, Sanofi, Seattle Genetics, SecuraBio, SkylineDX, Takeda, TeneoBio.
AD served as a consultant for Incyte, EUSA Pharma, Loxo and receives research support from Roche and Takeda.
BD Honoraria and Advisory Boards from Janssen and Sanofi.
All other authors have no conflicts of interest to declare.
Figures
















References
-
- Rajkumar SV Multiple myeloma: 2020 update on diagnosis, risk-stratification and management. Am J Hematol 95, 548–567 (2020). - PubMed
-
- Shah UA & Mailankody S Emerging immunotherapies in multiple myeloma. BMJ 370, m3176 (2020). - PubMed
-
- Costa LJ, et al. Daratumumab, Carfilzomib, Lenalidomide, and Dexamethasone With Minimal Residual Disease Response-Adapted Therapy in Newly Diagnosed Multiple Myeloma. J Clin Oncol, JCO2101935 (2021). - PubMed
-
- Diamond B, et al. Dynamics of minimal residual disease in patients with multiple myeloma on continuous lenalidomide maintenance: a single-arm, single-centre, phase 2 trial. Lancet Haematol 8, e422–e432 (2021). - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- P30 CA016087/CA/NCI NIH HHS/United States
- 6020-20/Leukemia and Lymphoma Society (Leukemia & Lymphoma Society)
- P30 CA 240139/U.S. Department of Health & Human Services | NIH | NCI | Division of Cancer Epidemiology and Genetics, National Cancer Institute (National Cancer Institute Division of Cancer Epidemiology and Genetics)
- P30 CA008748/CA/NCI NIH HHS/United States
- P30 CA240139/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
